
Abstract
Keywords
Introduction
ADHD is one of the most prevalent and most investigated mental disorders in children, with prevalence rates ranging from 3% to 6% (American Psychiatric Association [APA], 1994, 2000; Faraone, Sergeant, Gillberg, & Biederman, 2003; Kutcher et al., 2004). Since the mid-80s, there has been increased interest in the long-term course of this disorder. Longitudinal studies have shown that ADHD persists in many cases well into adulthood. Estimates suggest that approximately 15% to 65% (Faraone, Biederman, & Mick, 2006) of former childhood ADHD patients continue to fulfill diagnostic criteria in adulthood. The range of these estimations seems to depend on several independent factors, including the diagnostic criteria applied, the source of information used, the definition of remission and the ADHD subtype (Barkley, Fischer, Smallish, & Fletcher, 2002; Biederman, Mick, & Faraone, 2000; Faraone et al., 2006). Symptoms of inattention are more likely to persist into adulthood than symptoms of hyperactivity or impulsivity (Wilens, Faraone, & Biederman, 2004).
Recently, two comprehensive epidemiological studies have identified prevalence rates of adult ADHD of approximately 4% in epidemiological samples (Fayyad et al., 2007; Kessler et al., 2006), while in a clinical sample, a prevalence rate of approximately 17% was found (Montes, García, & Ricardo-Garcell, 2007). More males seem to be affected than females in both clinical and epidemiological samples. The gender ratio in childhood ADHD falls in the range of 9:1 to 4:1 (Cantwell, 1996), whereas adult samples have a more balanced gender distribution of approximately 1.5:1 (Fayyad et al., 2007; Kessler et al., 2006).
Adult ADHD patients frequently suffer from diverse symptoms, including a lack of concentration, inattention, forgetfulness, distractibility, erratic mood changes, and unhappiness caused by emotional overload (Barkley, Murphy, & Fischer, 2008). In addition, adults with ADHD have an increased risk of suffering from comorbid disorders, such as substance abuse and anxiety or mood disorders (for an overview, see Wilens, Biederman, & Spencer, 2002). In summary, adult ADHD is widely seen as a valid diagnosis (Faraone et al., 2000) and as a prevalent and serious condition that often affects multiple spheres of daily life (for a comprehensive overview, see Barkley et al., 2008)
Because it is commonly agreed that ADHD is a disorder of a neuropsychological nature (e.g., Barkley, 1997; Pennington & Ozonoff, 1996), there is a large body of research on neuropsychological impairments in ADHD patients. These include several qualitative and quantitative research syntheses published throughout the last 10 years on adult ADHD, some of which have focused on rather specific fields, such as attention, executive functioning, and intellectual performance (e.g., Boonstra, Oosterlaan, Sergeant, & Buitelaar, 2005; Bridgett & Walker, 2006). Other studies have attempted to paint a broader picture of the neuropsychological profile (Hervey, Epstein, & Curry, 2004; Schoechlin & Engel, 2005; Woods, Lovejoy, & Ball, 2002). Overall, adults with ADHD have been shown to perform worse on a number of neuropsychological measures compared with nonclinical controls. For instance, Schoechlin and Engel (2005) reported medium-sized effects for abstract verbal problem solving as well as focused and sustained attention in their meta-analysis of outcomes in 10 neurocognitive domains. The most considerable impairments, however, were found in the domain of verbal long-term memory (d = −.56). Hervey and colleagues (2004) found a similar pattern of results when they conducted a meta-analysis of the performance of adult ADHD patients and controls on subtests of multiple verbal memory tests. When compared with verbal long-term memory, group differences in visual long-term memory were consistently small (Hervey et al., 2004; Schoechlin & Engel, 2005).
These meta-analytic results are mostly in line with research in childhood ADHD, where most studies also reveal long-term memory impairments (e.g., Cahn & Marcotte, 1995; Cutting, Koth, Mahone, & Denckla, 2003; Egeland, Nordby Johansen, & Ueland, 2010; Kaplan, Dewey, Crawford, & Fisher, 1998). Although the stability of these impairments during development has been reported, their cause is still controversial. Is there a genuine memory impairment characterized by deficient retention or retrieval processes, or are the observed memory and learning deficits induced at the stage of encoding? Research on children with ADHD children has repeatedly demonstrated potential learning deficits. For example, Kaplan et al. (1998) assessed the learning and memory performance of ADHD patients on a number of verbal memory tests. The results indicated that children with ADHD performed worse on both learning and delayed recall subtests compared with nonclinical controls. However, when comparing the number of words recalled against the number of words learned in learning trials, no significant differences compared with healthy controls were found on these saving scores. The results of Kaplan et al. (1998) and similar findings based on visual material (Cahn & Marcotte, 1995) suggest that long-term memory performance deficits in ADHD patients might be traceable to problems in the initial learning of new material, that is, information that has been encoded into memory seems to remain intact, implying that retention processes are unaffected in at least childhood ADHD. This idea is also widely discussed in the research on adult ADHD (e.g., Hervey et al., 2004; Johnson et al., 2001; Seidman, Biederman, Weber, Hatch, & Faraone, 1998), but is seldom statistically demonstrated, although the necessary tests are commonly applied in research dealing with the neuropsychological performance of adult ADHD patients.
Although the aforementioned findings strongly point toward an encoding rather than a retention problem, it is at least conceivable that an additional retrieval impairment influencing long-term memory performance is present in ADHD. In this case, one would expect ADHD patients to perform poorly on free delayed recall tasks, but not on recognition tasks. Recognition tasks provide additional cues that facilitate the retrieval of information from memory. Thus, they are usually easier to accomplish than free recall tasks (Anderson, 2000). Under the assumption of hampered retrieval, ADHD patients should benefit even more from the retrieval aids recognition tests offer, such that smaller performance differences between ADHD and control adults than on free recall tasks would be expected. The literature on childhood and adult ADHD is inconsistent regarding the potential presence of a retrieval deficit. Some studies have found performance deficits on free recall tasks, but relatively intact recognition memory (e.g., Loge, Staton, & Beatty, 1990; Pollak, Kahana-Vax, & Hoofien, 2008), whereas other studies have found contradicting outcomes (e.g., Cutting et al., 2003; Dige & Wik, 2005). Thus, it remains an open question whether additional retrieval impairment exists in ADHD.
Several theoretical suggestions have been made with regard to the underlying factors that lead to long-term memory deficits in ADHD. The most influential theoretical model in the field is Barkley’s comprehensive theory (Barkley, 1997). Barkley argues that poor behavioral inhibition is the core deficit in ADHD. Secondary impairments in executive functions (e.g., working memory) are the consequences. The inability to encode material properly and to hold information in mind during the learning phases—especially complex or large amounts of information—is seen as the result of a behavioral inhibition deficit. Barkley’s view, however, was challenged by the work of Douglas and Benezra (1990), who stated that deficient self-regulation rather than behavioral disinhibition is the core deficit in ADHD. Self-regulatory or executive processes guide the organization and monitoring of information processing, attention, and effort. Following this approach, problems with memory acquisition should become most evident when self-regulated, effortful, and sustained performance is necessary. However, it is beyond the scope of this review to settle this controversial question.
In the present meta-analysis, we pursued three major goals. First, we sought to provide an update of the published literature on long-term memory deficits in adult ADHD and to replicate the findings of earlier meta-analyses on this topic (Hervey et al., 2004; Schoechlin & Engel, 2005). Because there have been as many new publications dealing with the memory performance of adults with ADHD since that time as were included in the most recent meta-analysis addressing this topic (Schoechlin & Engel, 2005), an update is important to validate the present findings. Furthermore, we sought to overcome, with a refined methodological approach, some of the limitations of previous meta-analyses, in which, for example, studies that did not introduce a healthy comparison group were included in the analyses and only a rough differentiation of the addressed memory domains was realized. We expected to find performance deficits in ADHD adults compared with healthy controls on measures of both verbal and visual long-term memory. In line with previous meta-analytic findings (Schoechlin & Engel, 2005; Hervey et al., 2004), these differences were predicted to be more pronounced with verbal material than with visual. We further hypothesized that differential performance between ADHD patients and controls would be measurable on tests of memory acquisition, again with larger effects in the verbal memory domain. Second, we wanted to investigate whether the long-term memory deficits observed in adults with ADHD are attributable to encoding problems, which showed to be plausible for childhood ADHD. Converging findings from research on memory impairments in childhood and adult ADHD suggest this, but to the best of our knowledge, it has never before been tested meta-analytically. We hypothesized that performance differences in long-term memory would reflect performance differences at the stage of encoding and not (additional) retrieval problems. Third, we anticipated that several study and sample characteristics would moderate the main effect of deficient long-term memory in adult ADHD. Potential moderators have been discussed in previous meta-analyses (Hervey et al., 2004; Schoechlin & Engel, 2005), but these have not been studied statistically as potential moderating variables.
Method
Literature Search
The English- and German-language literature concerning adult ADHD was searched using PsycINFO, MEDLINE, PubMed, ISI Web of Science, and Google Scholar. The search terms included adult, ADHD, ADD, hyperkinetic, attention-deficit disorder, memory, long-term, verbal, figural, visual, spatial, neuropsychological, neurocognitive, and executive as well as their German equivalents. Wildcards and the operator and were used where relevant. Additional articles were obtained by examining reference lists from review articles and the studies already identified in the search. Doctoral dissertations were included when they met the inclusion criteria. The search cutoff date was February 2013.
Inclusion and Exclusion Criteria
To determine study eligibility, full texts of all obtained studies were examined for several inclusion criteria. First, adults with ADHD had to be diagnosed using Diagnostic and Statistical Manual of Mental Disorders (3rd ed., rev.; DSM-III-R; APA, 1987), DSM-IV (4th ed.; APA, 1994), or DSM-IV-TR (4th ed., text rev.; APA, 2000) criteria or with comparably approved scales (e.g., Wender Utah Rating Scale; Ward, Wender, & Reimherr, 1993). As there is an ongoing debate about the validity of the age-of-onset criterion in DSM-IV, we decided to include studies in which ADHD was diagnosed without meeting the age-of-onset criterion and tested for potential moderating effects of the criteria used. Second, only studies comprising at least one test of long-term memory and a corresponding baseline measure of memory acquisition were included (for a list of commonly used tests of long-term memory, see Zakzanis, Leach, & Kaplan, 1999). This approach was considered to be necessary to address the research questions stated earlier. A descriptive listing of the tests and their specific trials/subtests that had to be conducted in a study to be included in the analyses is given below. Third, the performance of adults with ADHD on these measures had to be compared with a healthy control group (i.e., participants without previously existing diagnoses). Studies that compared ADHD patients with participants with other diagnoses only (e.g., major depression) were excluded. However, we considered studies in which ADHD patients were diagnosed with a comorbid disorder as long as ADHD was considered to be the primary diagnosis, and we tested for a potential moderating effect of present comorbidity in the ADHD group. In addition, the mean age of the participants had to be at least 18 years due to our focus on adult ADHD. Moreover, sufficient information for computing effect sizes had to be available either from the article itself or through the contact authors.
Obtained Studies
Twenty-four studies met our inclusion criteria. However, five of these had to be excluded due to usage of uncommon tests or experimental designs that were not comparable with other tests (this was the case for Abramovitch, Dar, Hermesh, & Schweiger, 2012; Knouse, Paradise, & Dunlosky, 2006; Miller, Nevado-Montenegro, & Hinshaw, 2012; Storm & White, 2010; White & Marks, 2004), leaving 19 studies suitable for inclusion in the present meta-analysis. Due to the stricter inclusion criteria that we applied, some of the studies included in previous meta-analyses on the same topic and some recently published studies had to be excluded either because they introduced no healthy comparison group or because the diagnosis of ADHD was not verified in all clinical subjects (this was the case for In de Braek, Dijkstra, & Jolles, 2011; Jenkins et al., 1998; Katz, Wood, Goldstein, Auchenbach, & Geckle, 1998). Collectively, the included 19 studies compared 827 adults with ADHD with 771 healthy controls on 14 different dependent variables (DVs) of interest. A representative study would have contained 40 subjects with adult ADHD who would have been approximately 31.64 years old with 14.20 years of education and 38 controls who would have been approximately 32.01 years old with 14.98 years of education (Table 1 presents detailed study and subject characteristics).
Study and Subject Characteristics.
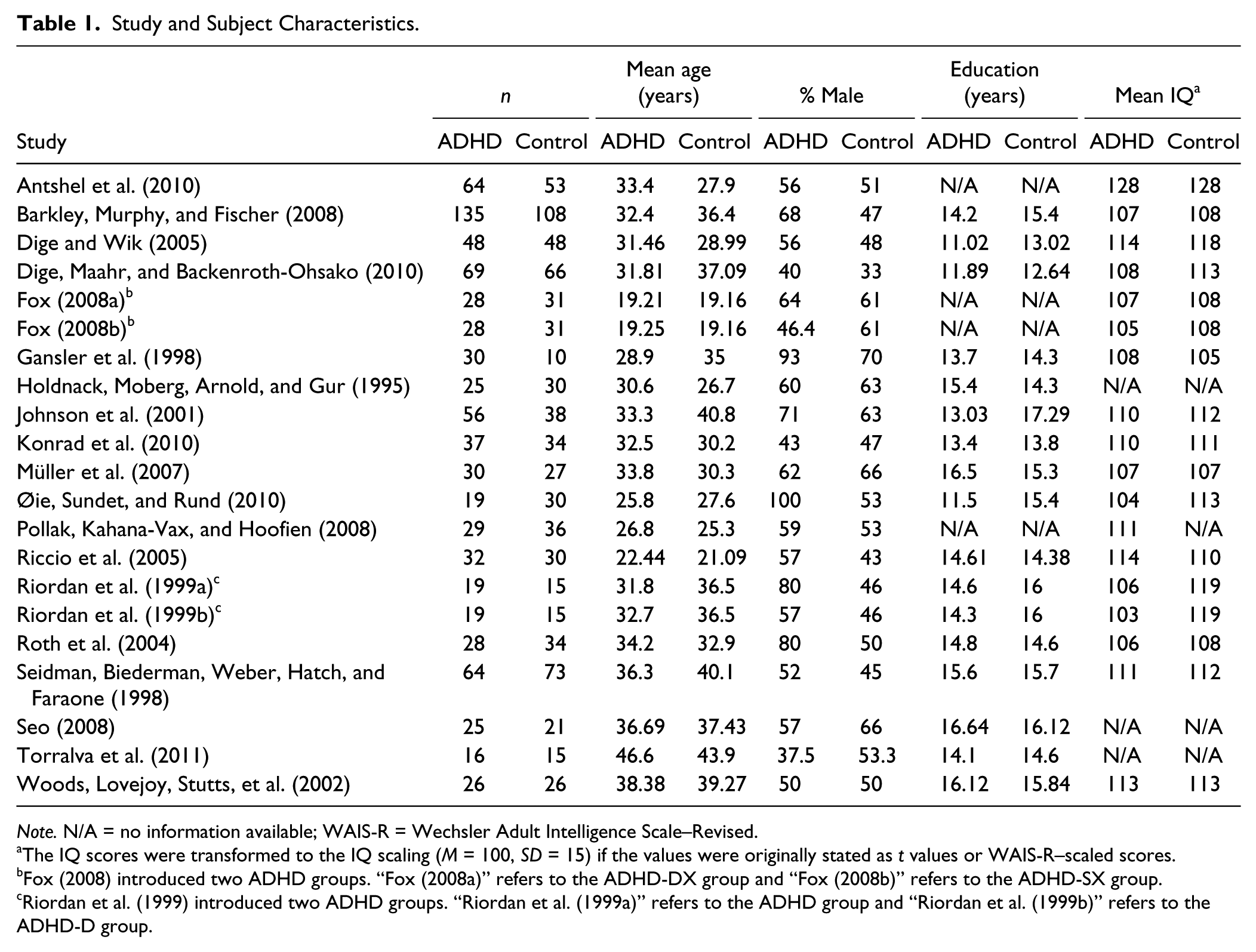
Note. N/A = no information available; WAIS-R = Wechsler Adult Intelligence Scale–Revised.
The IQ scores were transformed to the IQ scaling (M = 100, SD = 15) if the values were originally stated as t values or WAIS-R–scaled scores.
Fox (2008) introduced two ADHD groups. “Fox (2008a)” refers to the ADHD-DX group and “Fox (2008b)” refers to the ADHD-SX group.
Riordan et al. (1999) introduced two ADHD groups. “Riordan et al. (1999a)” refers to the ADHD group and “Riordan et al. (1999b)” refers to the ADHD-D group.
Obtained Measures
Dependent variables
Previous meta-analytic research has demonstrated that adults with ADHD perform rather heterogeneously in different domains of memory (Hervey et al., 2004; Schoechlin & Engel, 2005). To replicate these results, we adopted the classification system of Schoechlin and Engel (2005), and we performed separate analyses for verbal and visual memory. All memory tests utilized in the included studies were assigned to one of these two domains. In the verbal memory domain, the Rey Auditory Verbal Learning Test (AVLT; M. Schmidt, 1996), the California Verbal Learning Test (CVLT; Delis, Kramer, Kaplan, & Ober, 1987), the Paragraph subtest of the Learning and Memory Battery (LAMB; J. P. Schmidt & Tombaugh, 1995), and the Logical Memory subtest of the Wechsler Memory Scale–Revised (WMS-R; Wechsler, 1987) were included in the analyses. While the AVLT and the CVLT are based on a list-learning task, the Logical Memory subtest of the WMS-R and the Paragraph subtest of the LAMB examine participants’ ability to recall facts from orally presented stories. In the visual memory domain, the Rey–Osterrieth Complex Figure Test (ROCF; Osterrieth, 1944), the visual reproduction subtest of the WMS-R, and a modified version of the Visual Learning and Memory Test for Neuropsychological Assessment (Diagnosticum für Cerebralschädigung; mDCS; Dige & Wik, 2001) were included. All three tests ask the participants to reproduce abstract figures either with the help of wooden sticks or through drawing. For the ROCF, there are several scoring systems that provide criteria for the evaluation of participants’ drawings, including scores of the accuracy and organization of copy and recall. Because organization scores were not available in studies meeting the inclusion criteria, only accuracy ratings, which are conceptualized to capture visual-spatial memory performance (cf. Seidman et al., 1998), were included in the analyses. To ensure that the grouping of tests into the two memory domains was appropriate, we tested how far the study outcomes within one domain varied as a function of the test used. The results of a Q test based on a random-effects model with the pooled estimate of τ2 indicated that, in fact, homogeneous memory tests were pooled in both memory domains, Q(3) = 0.16, p = .984, for the verbal domain, and Q(3) = 5.44, p = .142, for the visual memory domain.
As the focus of the present meta-analysis was to investigate performance differences in long-term memory, only those subtests or indices of the used memory tests that introduced delayed recall intervals of sufficient length were of interest. Delay intervals of at least 20 min were considered adequate because they are applied most frequently in common measures of long-term memory. Thus, in the verbal memory domain, the dependent measures included the 20-min delayed free recall scores of the AVLT and the CVLT and the Logical Memory-II score of the WMS-R (30-min delayed free recall) as measures of long-term memory performance. In the visual memory domain, the 30-min delayed free recall scores of the Visual Reproduction subtest of the WMS-R (Visual Reproduction II) and the mDCS and the 20-min delayed accuracy score of the ROCF were entered into the analyses.
In addition, to test for performance differences in memory acquisition and recognition, corresponding memory subtests were coded. We chose those memory acquisition measures that were most frequently used in studies examining memory performances in adult ADHD, which allowed us to maximize the number of included studies. For all memory tests but the ROCF, we found the sum of correctly recalled items over the successive initial learning trial(s) to meet our requirements. Following Cahn and Marcotte (1995), for the ROCF, we considered the copy trial to equal a single learning trial so that the immediate recall score was used as a baseline measure. For the assessment of recognition memory, the corresponding recognition subtests were coded where available.
In the verbal memory domain, 19 studies contained data on delayed recall and corresponding measures of memory acquisition. Of these, only 9 studies also included data on recognition performance. In the visual memory domain, data on delayed recall and memory acquisition performance from 9 studies could be included in the analyses. Recognition performance in the visual memory domain could not be analyzed because a recognition test was used in only one study (Dige & Wik, 2005). In addition, cued-recall subtests were rarely used in the included studies both in the verbal and the visual memory domain. Thus, they were not incorporated into the analyses.
Study and subject characteristics
To assess the impact of certain study and subject characteristics on predicted performance differences between ADHD patients and healthy participants, each study was coded for several moderator variables. The selection was guided by the empirical findings outlined above and especially by the overviews of potential moderators given in previous reviews (Hervey et al., 2004; Schoechlin & Engel, 2005; Woods, Lovejoy, & Ball, 2002). Information concerning the following variables was collected: differences in referral sources for ADHD patients and control participants, age-of-onset criterion met, predominant ADHD subtype, presence of comorbid conditions, psychopharmacological medication status at the time of testing, and mean age of ADHD patients. Moreover, IQ score differences between the ADHD and the control group were calculated. The standardized mean difference in the educational level was computed using pooled standard deviations. Differences in the gender composition of the ADHD and the control samples were calculated by subtracting the percentage of male participants in the control group from the percentage in the ADHD group. In addition, as suggested by Lipsey and Wilson (2001), study descriptors such as type of publication (e.g., journal article or doctoral dissertation) and year of publication were coded. Table 2 presents the assigned moderator codes for each study.
Assigned Moderator Codes by Study.

Note. ADHD-C = ADHD, combined subtype; ADHD-H = ADHD, hyperactive subtype; ADHD-I = ADHD, inattentive subtype; N/A = predominant ADHD subtype not reported; DSM = Diagnostic and Statistical Manual of Mental Disorders (APA, 1987, 1994).
1 = journal article; 2 = book or book chapter; 3 = doctoral dissertation.
0 = age-of-onset criterion not met; 1 = age-of-onset criterion met.
0 = patients on medication at the time of testing; 1 = no history of medication for ADHD; 2 = at least a 12-hr wash-out phase for psychopharmacological medication; 3 = medication status at the time of testing not sufficiently reported.
0 = ADHD patients and controls recruited from the same source; 1 = ADHD patients and controls recruited from different sources; 2 = recruiting procedure not sufficiently reported.
0 = no comorbid disorders permitted; 1 = comorbid DSM Axis I disorders permitted; 2 = no information concerning the allowance for/the presence of comorbid conditions reported.
Fox (2008) introduced two ADHD groups. “Fox (2008a)” refers to the ADHD-DX group and “Fox (2008b)” refers to the ADHD-SX group.
Riordan et al. (1999) introduced two ADHD groups. “Riordan et al. (1999a)” refers to the ADHD group and “Riordan et al. (1999b)” refers to the ADHD-D group.
Statistical Methods
All data were analyzed using the computer program Comprehensive Meta-Analysis (Borenstein, Hedges, Higgins, & Rothstein, 2005) and the R-package metafor (Viechtbauer, 2010). Within the two memory domains, we assumed heterogeneous data sets because some of the included memory tests—though measuring the same psychological construct—differed with regard to the demands they put on participants. Thus, a random-effects model was chosen. For each measure, Cohen’s d, the standardized mean difference of the ADHD and the control group, was computed using pooled standard deviations (for the formulas used, see Borenstein, Hedges, Higgins, & Rothstein, 2009). We did not correct for sample size bias (Hedges & Olkin, 1985) because the resulting effect sizes deviated only marginally. In the following tables and figures illustrating the meta-analysis outcomes, a minus sign indicates that the ADHD group performed worse than the control group. Given the large number of statistical tests performed on basically the same studies, an adjusted alpha level of .01 was used for all analyses. To demonstrate the hypothesized moderating effects of the memory acquisition baseline and recognition memory, meta-regression and subgroup analyses were used (Borenstein et al., 2009). For all subgroup analyses, Q tests based on a random-effects model with pooled estimates of τ2 were used. Homogeneity of effect sizes was assessed by the Q statistic.
Prior to the main analyses, we inspected the data for outliers and influential cases within the two memory domains to rule out potential bias using the approach suggested by Viechtbauer and Cheung (2010). Missing data were also evaluated. There were a few missing values in some of the additionally coded variables concerning patient and study characteristics, and methodological factors described above because the required information was not available or was not given in sufficient detail in some studies. A twofold approach was used to address this issue: For discrete variables, missing values formed an additional category, which was also included in the moderator analysis, whereas for continuous variables, missing values were substituted with the mean of the available data weighted by sample size.
Another potential problem in meta-analyses is statistically dependent data due to multiple outcomes or comparisons within studies. Such dependent data structures have to be handled with caution because they can lead to an improper estimate of the standard error of the summary effect (Borenstein et al., 2009; Gleser & Olkin, 2009). In the present meta-analysis, only a relatively small number of the included studies were affected by this problem. Of the 19 studies, 2 included multiple comparisons between different ADHD groups and a shared control group, and 2 studies included multiple outcomes within the same memory domain derived from the same participants. Hence, their distorting effect might be expected to be negligible. Nevertheless, we chose to check this assumption by using the approach suggested by Hedges, Tipton, and Johnson (2010). As was expected, the sampling error estimations and the meta-analysis outcomes derived from this procedure were only marginally different from those obtained by the standard procedure described earlier. Thus, we decided to treat the statistically dependent outcomes as independent in the main analyses. This resulted in a total of 23 comparisons from the 19 studies in the verbal memory domain and 10 comparisons from the 9 studies in the visual memory domain. In the meta-analysis, k indicates the number of comparisons, not the number of studies.
Results
In the following section, the results will be reported separately for the verbal and visual memory domain. The meta-analyses of measures of long-term memory will be presented first, followed by an evaluation of the corresponding baseline measures for memory acquisition and, where possible, recognition memory. Subsequently, the results of the meta-regression analyses of the impact of memory acquisition on long-term memory will be reported. Finally, in cases of heterogeneous effect sizes, moderator analyses were conducted to shed light on potential moderators of the main long-term memory effect. Forest plots presenting standardized mean differences, standard errors, 99% confidence intervals, and p values for all measures are given in the respective paragraphs.
Verbal Memory
Delayed free recall
Figure 1 presents the meta-analytic outcomes for the verbal delayed free recall measures. Adults with ADHD performed significantly worse on delayed free recall tests compared with healthy controls (d = −0.49, p < .001). According to Cohen (1988), this could be considered a medium effect. The homogeneity test, however, revealed that a moderate amount of variance could not be accounted for by within-study variability, suggesting the presence of moderating variables, Q(22) = 59.50, p < .001, I2 = 63.03%.
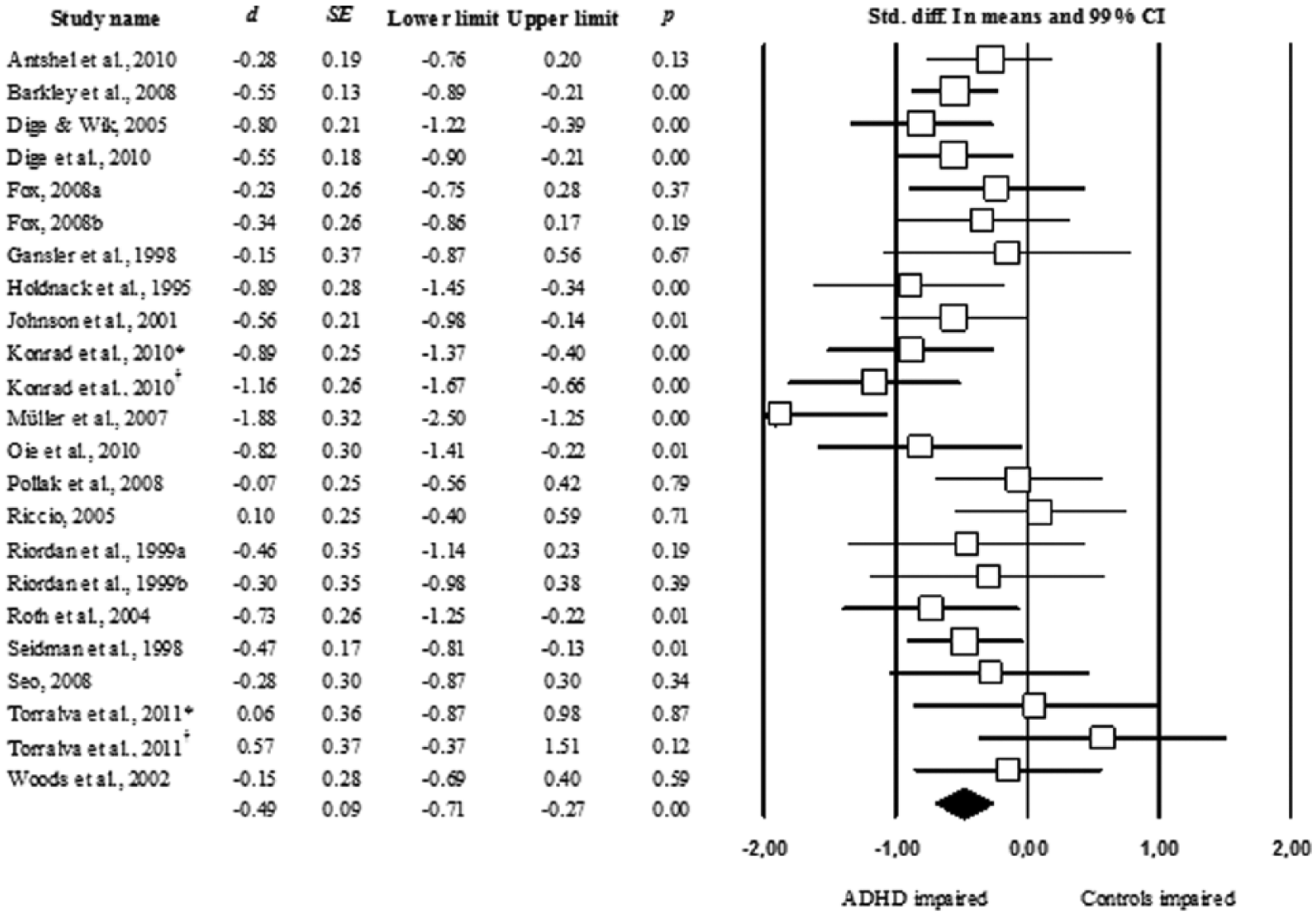
Forest plot of effect sizes derived from the verbal delayed free recall measures based on a random-effects model with pooled standard deviations. Konrad et al. (2010) and Torralva et al. (2011) conducted two verbal memory tests. An asterisk marks the results of the AVLT, while a dagger marks the results of the WMS-R.
Following the approach of Viechtbauer and Cheung (2010), we found one outlying and influential case (Müller et al., 2007) with a studentized deleted residual of z = −3.54, DFFITS = −0.71, Cook’s D = 0.35. 1 To examine the impact of this case on the meta-analytic results, a sensitivity analysis was conducted. With the case in question excluded from the analysis, the outcome would slightly decrease to d = −0.44, p < .001. In addition, the amount of heterogeneity would be reduced, Q(21) = 40.36, p = .007, I2 = 47.97%. To address the problem of publication bias, Rosenthal’s (1979) Fail-safe N was utilized. Fail-safe N quantifies the number of unpublished, nonsignificant studies necessary to reduce the obtained mean effect to a nonsignificant level. Fail-safe N reached well above the set 5k + 10 criterion (where k indicates the number of comparisons included in the meta-analysis) of 125 unpublished studies, with Fail-safe N = 283, indicating that the results are not distorted by the effect of publication bias.
Memory acquisition baseline
Healthy controls outperformed adults with ADHD to an even greater extent in memory acquisition, d = −0.58, p < .001. Again, the Q statistic indicated a sizable amount of heterogeneity, Q(22) = 73.05, p < .001, I2 = 69.88%. 2 Figure 2 presents the meta-analytic outcomes for the verbal memory acquisition measures.

Forest plot of effect sizes derived from the verbal memory acquisition measures based on a random-effects model with pooled standard deviations. Konrad et al. (2010) and Torralva et al. (2011) conducted two verbal memory tests. An asterisk marks the results of the AVLT, while a dagger marks the results of the WMS-R.
To test the hypothesis that the long-term memory performance deficits of ADHD adults are (at least partially) attributable to deficiencies present at the stage of memory acquisition, a meta-regression was performed. The standardized performance differences on memory acquisition subtests were added as a covariate to the random-effects model with performance on delayed recall measures as the dependent variable and group assignment (ADHD/control group) as the independent variable (IV). On the assumption that the performance on memory acquisition measures influences the performance on delayed recall trials, one would expect the covariate to explain a significant amount of variance in the DV. The results demonstrated that performance on memory acquisition subtests strongly affected the delayed recall performance differences, Q(1) = 36.47, p < .001. In detail, the bigger the performance difference in the stage of memory acquisition, the bigger the performance difference in long-term memory, as indicated by the regression coefficient, β = 0.69, z = 6.04, p < .001 (see Figure 3). As a measure of explained variance, an analogue to R2, which was defined as the proportion of the total between-study variance explained by the model (Borenstein et al., 2009), was computed. It showed that 95.9% of the heterogeneity in the delayed recall outcomes (indicated by I2) could be explained by differences in memory acquisition performance. 3 Hence, long-term memory performance deficits in adults with ADHD are strongly influenced by deficits already present in the stage of memory acquisition.
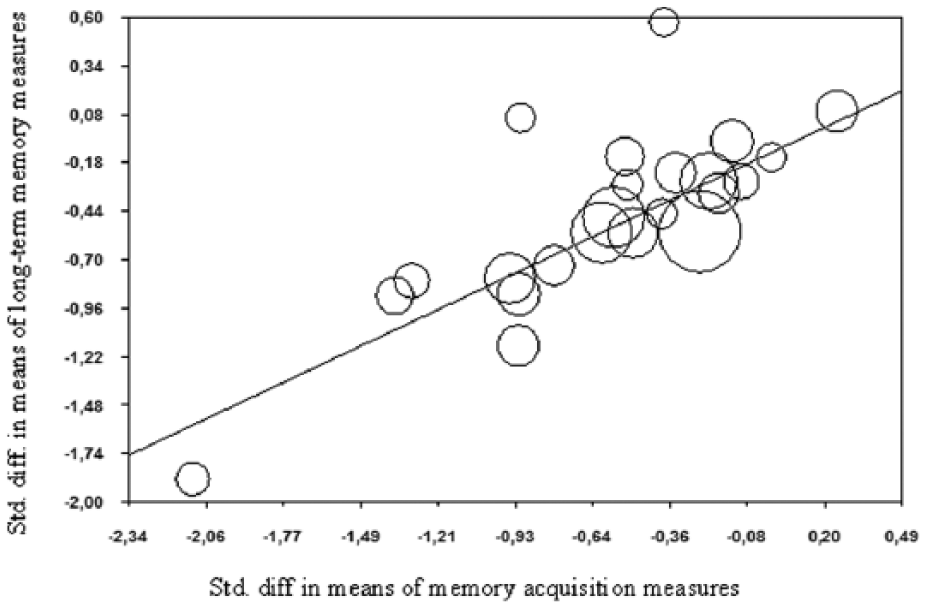
Regression of standardized mean differences of verbal long-term memory measures on standardized mean differences of verbal memory acquisition measures (mixed-effects model with pooled estimates of τ2). A minus sign indicates that the ADHD group performed worse than the control group.
Recognition memory
Of the 19 studies included in the verbal memory domain, 9 yielded information on recognition memory. Figure 4 presents the meta-analysis’ outcomes for the verbal recognition measures. Comparable with the previously reported results, the ADHD group performed worse than the healthy control group, d = −0.51, p = .002. Again, the Q statistic indicated that a considerable amount of heterogeneity was present, Q(7) = 24.76, p = .002, I2 = 67.69%.
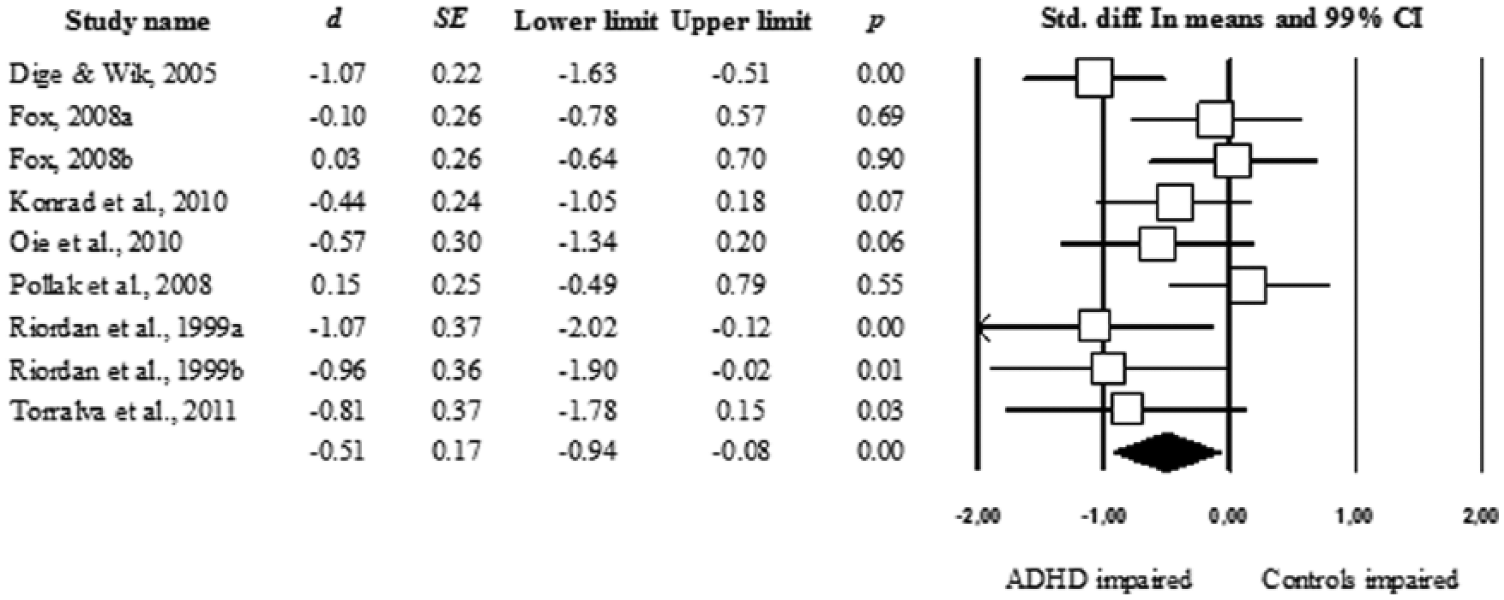
Forest plot of effect sizes derived from the verbal recognition measures based on a random-effects model with pooled standard deviations.
To investigate to what extent performance deficits in adults with ADHD on delayed recall tasks were not only due to deficient memory acquisition processes (as shown above) but also determined by deficient retrieval processes, we contrasted the effect sizes derived from delayed recall subtests with the recognition effect sizes and tested the null hypothesis that the difference was zero, an approach analogous to a t test with paired samples. 4 The results indicate that the null hypothesis could not be rejected, d = −0.05, z = −0.36, p = .72, suggesting that effect sizes obtained from free recall and recognition trials did not vary significantly. Thus, based on these findings, there is no evidence for an additional retrieval deficit in adult ADHD.
Moderator analyses
None of the following covariates had a significant impact on the main effect given the adopted alpha level of .01: presence of comorbid conditions in the ADHD group, Q(2) = 5.46, p = .065; year of publication, Q(1) = 0.62, p = .805; type of publication, Q(2) = 0.71, p = .703; difference in referral sources, Q(2) = 1.47, p = .480; age of onset, Q(1) = 0.01, p = .931; predominant ADHD subtype, Q(3) = 8.13, p = .043; medication status at the time of testing, Q(3) = 4.95, p = .176; IQ score, Q(1) = 0.08, p = .778; mean age of the ADHD patients, Q(1) = 0.23, p = .631, difference in educational level; Q(1) = 0.92, p = .338; and difference in gender composition, Q(1) = 0.36, p = .548.
Visual Memory
Delayed free recall
Figure 5 presents the meta-analytic outcomes for the visual delayed free recall measures. We found a small, nonsignificant performance difference in visual long-term memory of ADHD adults and healthy controls, d = −0.36, p = .108. A high amount of heterogeneity was present as indicated by the Q statistic, Q(9) = 68.61, p < .001, I2 = 86.88%.
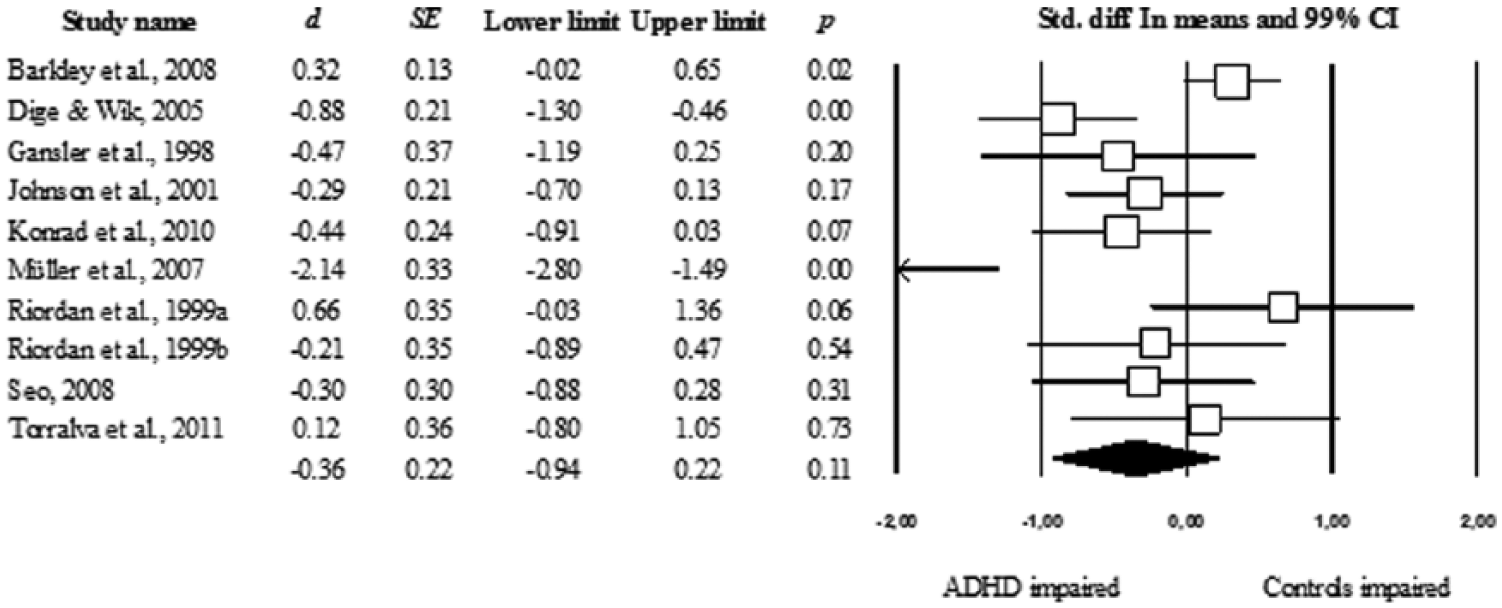
Forest plot of effect sizes derived from the figural delayed free recall measures based on a random-effects model with pooled standard deviations.
Again, we examined the data for outlying and influential cases. Here, too, we found the study of Müller et al. (2007) to be an outlying and an influential case with a studentized deleted residual of z = −3.66, DFFITS = −1.20, Cook’s D = 0.65. The results of a sensitivity analysis suggested that this study had a substantial impact on the outcomes. A deletion of this case leads to a considerable decrease in the effect size to d = −0.18, p = .303. In addition, the amount of heterogeneity would be reduced, Q(8) = 32.99, p < .001, I2 = 75.75%. Fail-safe N based on all 10 comparisons did not reach the critical value of the 5k + 10 rule, Fail-safe N = 12, critical value = 60. Thus, the present findings have to be judged with the caveat in mind that their liability to publication bias cannot be ruled out.
Memory acquisition baseline
Figure 6 presents the meta-analytic outcomes for the visual memory acquisition measures. Adults with ADHD did not significantly differ from healthy controls in their performance on subtests measuring memory acquisition, d = −0.12, p = .567. The Q statistic indicated a high amount of heterogeneity, Q(9) = 55.95, p < .001, I2 = 83.91%. When excluding the outcomes of Müller et al. (2007), altered effect sizes and heterogeneity values were found, d = −0.05, p = .717, and Q(8) = 23.57, p = .003, I2 = 66.07%.

Forest plot of effect sizes derived from the figural memory acquisition measures based on a random-effects model with pooled standard deviations.
The outcome of the meta-regression analysis also indicated that in the visual memory domain, the performance on delayed recall tests was significantly influenced by performance differences in memory acquisition, Q(1) = 45.61, p < .001. Again, the regression coefficient implied that the bigger the performance difference in the stage of memory acquisition, the bigger the performance difference in long-term memory, β = 0.93, z = 6.75, p < .001 (see Figure 7). R2, as a measure of the explained between-study variance, showed that 64.2% of the heterogeneity in the delayed recall outcomes (indicated by I2) was explained by the differences in memory acquisition performance. 5
In summary, our findings showed that there were no significant performance differences present in measures of memory acquisition. Notwithstanding, these differences—small as they were—clearly influenced differences in long-term memory performance, as demonstrated by the meta-regression analysis.

Regression of standardized mean differences of figural long-term memory measures on standardized mean differences of figural memory acquisition measures (mixed-effects model with pooled estimates of τ2). A minus sign indicates that the ADHD group performed worse than the control group.
Moderator analyses
The study descriptor “age-of-onset criterion met” had to be dropped from the analyses because in only one study was the age-of-onset criterion not met (Barkley et al., 2008). In the visual memory domain, only the “presence of comorbid conditions in the ADHD group” had a significant impact on the main effect, Q(2) = 11.26, p = .004. The biggest performance differences resulted from studies in which no information was reported regarding whether ADHD patients with comorbid disorders were included, followed by studies in which strict exclusion criteria were applied such that no comorbid conditions were permitted. The smallest differences were found for studies with less strict inclusion criteria, which allowed for DSM Axis I disorders. Post hoc analyses showed that the two comparisons reached significance: The effect size based on the group of studies not stating the presence of patients with comorbid disorders differed significantly from the effect size derived from studies allowing for specific comorbidities, Q(1) = 11.23, p = .001, and from the effect size derived from studies allowing for no comorbidities, Q(1) = 17.17, p < .001. No other covariate reached significance on the adopted alpha level of .01: year of publication, Q(1) = 0.19, p = .659; type of publication, Q(2) = 1.24, p = .539; difference in referral sources, Q(1) = 0.66, p = .416; predominant ADHD subtypes, Q(3) = 1.74, p = .627; medication status at the time of testing, Q(3) = 6.05, p = .109; IQ score differences, Q(1) = 1.90, p = .168; mean age of ADHD patients, Q(1) = 0.20, p = .652; difference of educational level, Q(1) = 0.01, p = .926; and difference in gender composition, Q(1) = 2.18, p = .139.
Discussion
In this meta-analysis, we examined underlying mechanisms that may contribute to long-term memory impairments in adult ADHD while validating the findings of earlier meta-analyses and providing evidence for a long-term memory deficit in adult ADHD. Moreover, we investigated the moderating influence of certain study and patient characteristics on the main findings.
Long-Term Memory Performance
Consistent with our hypothesis, and in line with previous research (e.g., Schoechlin & Engel, 2005), we found a long-term memory performance deficit in adults with ADHD compared with healthy controls, an effect that varied in size between the verbal and visual memory domain. On verbal long-term memory tests, adults with ADHD were clearly outperformed by nonclinical controls, resulting in a medium-sized effect of d = −0.49. This effect was robust to the potentially distorting effects of influential cases, as was demonstrated by sensitivity analyses, and was not influenced by publication bias. For the visual memory domain, a different picture emerged. We found a nonsignificant effect (d = −0.36) that was not only comparable in size with previous findings (Hervey et al., 2004; Schoechlin & Engel, 2005) but also strongly dependent on the outcome of one single study. With this particular case excluded from the analysis, the outcome was considerably reduced in size (i.e., d = −0.18). In addition, we showed that the visual memory effect might be influenced by publication bias.
When discussing potential limitations of these findings, we must take into consideration that analyses in the visual memory domain were based on only 10 comparisons. Most likely, this has resulted in low statistical power given that only a small effect could have been anticipated (cf. Hedges & Pigott, 2001). In addition, with respect to publication bias, we should keep in mind that the small number of included studies and the anticipated small effect led to a small Fail-safe N (cf. Rosenthal, 1979). Another influence might have been the considerable amount of heterogeneity that we found in both memory domains. Especially in the visual memory domain, we found a considerable amount of between-study variation (I2 = 86.88%); consequently, confidence intervals were large, and it was even more unlikely that the predicted small effect would reach significance (cf. Borenstein et al., 2009). There are different possible explanations for this heterogeneity in our analyses. As our sensitivity analyses revealed, a significant amount of between-study variability in both memory domains was induced by the deviant results of a single study (Müller et al., 2007). By temporarily removing this case, heterogeneity could be substantially reduced in both memory domains. Another possible explanation for the between-study variation is the grouping of heterogeneous memory tests. Prior to our analyses, we examined whether this was the case by statistically comparing the effect sizes derived from each memory test within each of the two domains. However, we found no significant impact of the type of test on the meta-analytic outcomes. Thus, there is no evidence in our data that the present heterogeneity was due to an unreasonable grouping of memory tests. This finding is in line with the results of various validation studies showing the close correlational association of certain memory tests (e.g., Delis, Cullum, Butters, Cairns & Prifitera, 1988). Finally, heterogeneity often occurs because of the presence of study-level variables that moderate the main effect. We will return to this issue below.
Encoding and Retrieval Performance
In the literature on long-term memory impairments in ADHD, there are two main competing views regarding the question of which factors may cause them. Some researchers argue that observed long-term memory deficits are, in fact, learning deficits; the impaired long-term memory performance results from problems at the stage of encoding and not from deficient storage or retrieval of information (e.g., Cahn & Marcotte, 1995; Kaplan et al., 1998; Seidman et al., 1998). Opposing this hypothesis, other researchers believe that (additionally) retrieval processes might be adversely affected in ADHD (e.g., Loge et al., 1990; Pollak et al., 2008).
In the present meta-analysis, we found that adults with ADHD performed, in part, significantly worse than nonclinical controls on memory acquisition measures. This was the case only for verbal tests, where an effect even larger than the long-term memory effect was revealed (d = −0.58). However, for visual material, no significant difference was found (d = −0.12). Further analyses demonstrated that performance differences on memory acquisition trials had a highly significant impact on the performance difference on free recall trials. In detail, the bigger the performance difference at the stage of encoding, the bigger the difference in long-term memory performance. Thus, our results strongly support the hypothesis of deficient encoding processes as the cause of memory impairments in ADHD. Furthermore, corroborative evidence was gained by comparing the recognition and recall performances of ADHD patients and controls. We found that the performance deficits of adult ADHD patients on recall and recognition trials were of similar size. Thus, in our data, there is no indication of hampered retrieval processes being present in adult ADHD. In fact, consistent with our hypotheses, our findings provide evidence that retention and retrieval processes are unaffected, whereas impaired encoding processes lead to the observable deficits in long-term memory performance in adult ADHD.
These findings are, for the most part, in line with evidence derived from research in childhood ADHD, where similar patterns of results were found for both verbal and visual long-term memory. In the study of Cahn and Marcotte (1995), for instance, the ADHD group performed below age-appropriate norms on the immediate and delayed recall trials of the ROCF, but displayed normal rates of forgetting. In addition, Cutting and colleagues (2003), who reported in their more recent work performance metrics of ADHD and nonclinical children on various subtests of the children’s version of the CVLT, found that children with ADHD showed impairments on both delayed recall and recognition measures, but no differences regarding the rate of forgetting. Taken together, the findings concerning childhood ADHD and the outcome of the present meta-analysis agree that the long-term memory impairment in ADHD is attributable to deficient initial learning and not to impaired retention or retrieval of information.
Nevertheless, what determines this “encoding deficit” and why it predominantly occurs with verbal material remain open questions. Of course, a number of cognitive processes affect the encoding of information into memory, such as attention, executive functioning, working memory, usage of learning, or mnemonic strategies, and so on. Of these cognitive domains, Barkley (1997) and Pennington and Ozonoff (1996) suggest dysfunctions in executive functioning, such as inhibition, planning, fluency, working memory, and set shifting, to be the core deficit in ADHD (for meta-analytic evidence, see Boonstra et al., 2005; Hervey et al., 2004; Willcutt, Doyle, Nigg, Faraone, & Pennington, 2005). Hence, impaired acquisition in long-term memory might reflect an underlying executive core deficit in, for instance, the effective organization of stimuli. The phenomenon of diverging impairments in verbal and visual long-term memory is a stable effect found in a number of meta-analyses, but the literature on neuropsychological functioning in adult ADHD does not provide a conclusive explanation for this effect. One frequently discussed idea is that the two modality-specific slave systems of Baddeley’s model of working memory (Baddeley & Hitch, 1974) may play a crucial role in explaining this phenomenon. Performance deficits on verbal memory tasks may arise from the insufficient allocation of attention to the phonological loop. As a result, the processing of verbal information may be disrupted such that phonological or semantic features of the material to be learned are neglected and thus not entirely encoded into memory (cf. Hervey et al., 2004). There is only anecdotal evidence for this hypothesis. For example, a similar pattern of results is observed in the verbal fluency performances of adults with ADHD with verbal and visual cues. In their meta-analysis, Hervey et al. (2004) found that adults with ADHD performed worse compared with controls on such tasks when only verbal cues were available to generate verbal responses. In contrast, no performance difference occurred when a visual picture was allowed as a cue. Certainly, this idea is in need of further investigation, but it offers an interesting starting point for a detailed examination of the phenomenon.
As an additional consequence, opportunities to apply potentially helpful learning strategies may also be missed when verbal information is only incompletely encoded. In verbal list learning tests, such as the AVLT and the CVLT, strategies such as semantic clustering are indeed effective aids. It should be noted that ADHD patients are known to use such effortful learning strategies less spontaneously (e.g., Egeland et al., 2010). Thus, it could be concluded that the higher the demand for organization and mnemonic strategies that the memory task places on the subjects, the bigger the performance differences. This has been repeatedly demonstrated in ADHD children with verbal as well as visual material (e.g., Douglas & Benezra, 1990). Because all of the memory tests that were used in the included studies require effortful processing, it was unfortunately not possible to address this hypothesis in our meta-analysis.
In conclusion, it remains an open question as to what roles impaired executive functioning, working memory, self-regulation, or effort (or a combination of these) may play in contributing to the learning deficits observed in adult ADHD. However, as has been recently stated by Nigg (2005), it is unlikely that one single theory can account for the range of phenomena in ADHD. Instead, a continuing integration of models from various fields of research might be necessary to gain further insights into the etiology of this disorder.
Moderating Variables
In our moderator analyses, only the covariate “presence of comorbid conditions in the ADHD group” had a significant influence on the main effect, but only in the visual memory domain. 6 Differences in long-term memory performances were significantly more pronounced in studies that did not state explicitly whether ADHD patients with comorbid disorders were compared with both studies that allowed for specific comorbidities and studies that explicitly did not. As the aforementioned outlying case (Müller et al., 2007) is the only study in the “omission group” in the visual memory domain, this effect seems to be an artifact. Interestingly, no significant difference in effect sizes were found between studies that included patients with comorbid DSM Axis I disorders and studies that explicitly did not. Thus, long-term memory performance in adult ADHD seems to be unaffected by the presence of comorbid disorders, unlike global intellectual functioning, which has been shown to be impaired in adults with ADHD suffering from comorbid disorders (for an overview, see Bridgett & Walker, 2006). Apart from this, no other covariate served as a moderator of the long-term memory performance differences between ADHD adults and controls, although primary research would have suggested that certain factors, such as IQ (e.g., Fujii, Lloyd, & Miyamoto, 2000), sex- and age-related differences (e.g., Bleecker, Bolla-Wilson, Agnew, & Meyers, 1988), medication at the time of testing (Advokat, 2010), ADHD subtype (cf. Woods, Lovejoy, & Ball, 2002), or referral source (cf. Boonstra et al., 2005), might be expected to affect our results. Analyzing our data, two probable reasons for this lack of difference could be identified. First, most of the covariates had only very little variation present, that is, on several categorical variables, most cases (i.e., studies) fell in only one of the defined categories, and on most continuous variables, only a restricted range of scores was present. In addition, regarding some variables (e.g., predominant ADHD subtype), only few studies provided sufficient information to be able to categorize them reliably. This resulted in a relatively high number of studies in the respective missing value category. Thus, the moderator analyses may have been compromised by restriction of range; this, in turn, may have lowered the probability of finding significant correlations. Moreover, the moderator analyses may have suffered from low statistical power (Hedges & Pigott, 2004). Especially in the visual memory domain, where only 10 comparisons could be included, the ratio of studies to covariates might have been too small to make the analysis meaningful (cf. Borenstein et al., 2009). Therefore, it seems advisable to treat the findings of the moderator analyses with caution.
Limitations
After having outlined some limitations regarding the various research questions that we addressed in the respective paragraphs of the “Discussion” section, we want to address some global methodological issues of our meta-analysis. First, when interpreting our data, one has to keep in mind that the sample of studies that we were able to include was rather small—especially in the visual memory domain. Thus, it seems reasonable to treat the outcomes in the visual memory section with the necessary caution, even more so when considering that they might be influenced by publication bias. Another limitation might be the large amount of heterogeneity that we found within the two memory domains. We addressed this issue by ruling out that we had clustered immanently heterogeneous memory tests and by conducting a moderator analysis to identify potential influencing factors. The results of the moderator analyses, nonetheless, should be seen as being explorative rather than conclusive because they are based on limited data. Finally, one has to bear in mind that we face a methodological problem when examining differences in performance patterns of verbal versus visual memory tasks in adult ADHD. As L. J. Chapman and J. P. Chapman (1978) pointed out, psychometric properties, such as the tests’ reliability and the distributions of item difficulty, alter the probability of finding a differential deficit in performance regardless of whether a differential deficit of ability exists. L. J. Chapman and J. P. Chapman suggest matching tests on the mentioned parameters. In the case of meta-analytic research, we can only draw on data already collected; however, in our meta-analysis, clusters of various tests with varying psychometric properties are combined for measuring the same construct.
Conclusion
In sum, in this meta-analysis, we showed a long-term memory performance deficit in adult ADHD patients. In doing so, we validated the existing meta-analytic findings concerning that hypothesis based on an up-to-date body of research using a refined methodological approach by applying stricter inclusion criteria and analyzing memory tests more differentially. We were able to include the outcomes of 12 new publications in our analyses, while some of the studies that were entered into previous meta-analyses had to be excluded due to the stricter inclusion criteria we applied. As a result, conclusions regarding the issue in question can now be drawn on a broader and sounder basis.
Moreover, the present meta-analysis was the first to perform a statistical moderator analysis on the topic of long-term memory functioning in adult ADHD, and, despite certain limitations, basic indications regarding the influence of controversially discussed patient characteristics on memory performance differences of ADHD adults and controls can be derived. Future studies should report relevant information concerning study and patients’ characteristics—especially the predominant ADHD subtype in the study sample, the presence of comorbid conditions in ADHD patients, and years of education of the ADHD and control sample—in sufficient detail. Furthermore, future meta-analyses on this issue will hopefully have access to a greater number of studies. Both advancements would put them in the position to carry out more reliable moderator analyses.
Most importantly, this article is the first meta-analysis to shed light on the underlying mechanisms that may cause the frequently reported long-term memory deficits observed in adult ADHD. Memory problems are thought to be one of the most reported symptoms in adult ADHD. Both the DSM-IV-TR (APA, 2000) and the DSM-V (5th ed.; APA, 2013) contain references to memory impairments. The effect is well documented by a large number of neuropsychological studies, and this meta-analysis also comprehensively confirmed it. Based on the present findings and, for the most part, in line with previous research, it seems that the observed long-term memory deficits in adult ADHD are instead learning deficits induced at the stage of encoding of material to be learned. In contrast, no (additional) retention or retrieval problems contributed to the observable long-term memory impairment. Unfortunately, it was not possible to conduct a conventional mediational analysis (e.g., Baron & Kenny, 1986) to establish the causal link between encoding and long-term memory deficits because this approach requires a specific data structure, which was not available from data reported in the included studies (e.g., separate raw data of the respective mediator and the dependent variables for each group). However, because we could show that up to 95% of the variation of study-level effect sizes for long-term memory performance could be explained by performance at the stage of memory acquisition, there is still strong evidence corroborating our hypotheses. Nonetheless, future studies should close this methodological gap by implementing mediational analysis sensu Baron and Kenny (1986) or Structural Equation Modeling, to establish the causal chain. Of similar value would be a meta-analysis to investigate whether a similar pattern of results is observable in childhood ADHD. This would also add to the developmental understanding of neuropsychological functioning in ADHD.
Our results reveal impaired memory acquisition, but spared memory retention and retrieval. Hence, long-term memory deficits in ADHD might reflect a dysfunction in processes underlying memory acquisition, such as attention, executive functioning, working memory, self-regulation, or motivation (cf. Barkley et al., 2008). To be able to make more precise suggestions for neuropsychological treatments, the pivotal question that has to be answered by future research is which underlying processes determine the demonstrated encoding problems in adult ADHD. Given the wealth of theoretical and empirical perspectives on the etiology of the disorder, a number of encouraging starting points can be derived. It can be assumed that several approaches will contribute to broadening our understanding of the neuropsychology of adult ADHD.
Footnotes
Acknowledgements
We want to thank Niels Dige, Petra P. M. Hurks, Andreas Konrad, Bernhard W. Mueller, Bedriye Öncü, Yehuda Pollak, Cynthia A. Riccio, Teresa Torralva, and Steven P. Woods for providing additional data or information on their studies for this meta-analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.