
Abstract
While an increasing number of girls and women are being identified with autism, we know little about the health of reproductive-aged autistic women. Our objectives were to (1) describe health characteristics of reproductive-aged autistic women who could potentially become pregnant and (2) compare these characteristics with those of non-autistic women. We conducted a population-based cross-sectional study using 2017–2018 administrative health data from Ontario, Canada. A total of 6,870 fifteen- to 44-year-old autistic women were identified and compared with 2,686,160 non-autistic women. Variables of interest included social determinants of health (neighborhood income, residential instability, material deprivation, rurality), health (co-occurring medical and psychiatric conditions, use of potentially teratogenic medications, history of assault), and health care factors (continuity of primary care). Overall, reproductive-aged autistic women had poorer health compared with non-autistic women, including increased rates of material deprivation, chronic medical conditions, psychiatric conditions, use of potentially teratogenic medications, and history of assault. These findings highlight the need for health interventions tailored to the needs of reproductive-aged autistic women.
Lay abstract
While an increasing number of girls and women are being identified with autism, we know little about reproductive-aged autistic women’s health. This study used administrative data from Ontario, Canada, to compare the health of reproductive-aged autistic women with non-autistic women. Overall, reproductive-aged autistic women had poorer health compared with non-autistic women, including increased rates of material deprivation, chronic medical conditions, psychiatric conditions, history of assault, and use of potentially teratogenic medications (i.e. drugs that can be harmful to the development of an embryo or fetus). These findings suggest that there is a need for health interventions tailored to the needs of reproductive-aged autistic women.
Keywords
Autism is a neurodevelopmental condition characterized by differences in social communication and restricted, repetitive patterns of behavior (American Psychiatric Association, 2013). Occurring in approximately 1% of the population (Baio et al., 2018; Kim et al., 2011), autism has historically been described as a predominantly male condition, with a male: female ratio approximating 3:1 (Loomes et al., 2017). However, autistic girls and women are frequently underrecognized due to sex and gender differences in the presentation of features of autism (Lai et al., 2015). For instance, autistic women may be better able than men to “camouflage” their social communication difficulties, that is, either hide behaviors that might be viewed as socially unacceptable and/or imitate others’ social behavior (Lai et al., 2015). Consequently, many autistic girls and women report pervasive unmet care needs (Baldwin & Costley, 2016; Lum et al., 2014; Tint & Weiss, 2018).
Perhaps reflective of improved awareness of a “female phenotype,” autism has increasingly been identified in girls and women in recent years (Jensen et al., 2014; Kočovská et al., 2012; Lai & Baron-Cohen, 2015). A large percentage of these women are in their reproductive years (i.e. 15–44 years of age) with desires for sexual relationships similar to their non-autistic peers (Dewinter et al., 2017; Gilmour et al., 2012). Nearly half of all pregnancies are unplanned (Sedgh et al., 2014), and health before pregnancy has been shown to influence risks for adverse reproductive, maternal, and neonatal outcomes (World Health Organization, 2012). Recognizing this, interventions now focus on the health of all reproductive-aged women, regardless of their pregnancy intentions (World Health Organization, 2012). Growing evidence suggests that such interventions lead to better reproductive, maternal, and neonatal outcomes, including improved fertility and lower rates of pregnancy complications, preterm birth, congenital anomalies, and maternal and neonatal mortality (H. K. Brown et al., 2017; World Health Organization, 2012). While we know little about autistic women’s pregnancy outcomes and experiences, recent research suggests that they are at increased risk of medical and psychiatric complications (Gardner et al., 2016; Kassee et al., 2020; Pohl et al., 2020; Rogers et al., 2017; Sundelin et al., 2018). Understanding the health profiles of reproductive-aged autistic women is a prerequisite for improving their perinatal care and preventing adverse maternal and neonatal outcomes.
A range of modifiable risk factors are associated with adverse reproductive, maternal, and neonatal outcomes. These factors include social determinants of health, chronic medical conditions, psychosocial concerns, potentially teratogenic medications, and access to preventive health care (World Health Organization, 2012). Little is known about the health of reproductive-aged autistic women. However, autistic women encounter challenges obtaining and maintaining employment (Taylor et al., 2015, 2019) and, consequently, experience high rates of poverty (Nicolaidis et al., 2015). Many medical and psychiatric conditions occur more frequently in autistic women than in the general population (Croen et al., 2015; Joshi et al., 2013; Lugnegård et al., 2011), and autistic women are at increased risk of sexual victimization and financial exploitation (K. R. Brown et al., 2017; Brown-Lavoie et al., 2014; Ohlsson Gotby et al., 2018). High rates of medication use (Buck et al., 2014; Esbensen et al., 2009; Lake et al., 2012; Sundelin et al., 2018; Vohra et al., 2016; Zerbo et al., 2019) and poor access to primary health care (Nicolaidis et al., 2013; Zerbo et al., 2019) are also common among autistic women.
Small sample sizes limit the generalizability of current research (Kassee et al., 2020). Few existing sex-specific, population-based studies permit identification of health characteristics of reproductive-aged autistic women because findings are not disaggregated by age (Cawthorpe, 2017; Croen et al., 2015; Rydzewska et al., 2018, 2019). In the current study, we used population-based data from Ontario, Canada, to (1) describe the health characteristics of reproductive-aged autistic women who could potentially become pregnant and (2) compare these characteristics with those of non-autistic women.
Method
We studied the health characteristics of autistic and non-autistic women aged 15 to 44 years as of October 1, 2017, in Ontario, Canada, using administrative health data. We included all women of reproductive age, regardless of their pregnancy status, excluding women with a prior hysterectomy (who could not later become pregnant). The use of these data was authorized under section 45 of Ontario’s Personal Health Information Protection Act, which does not require review by a Research Ethics Board.
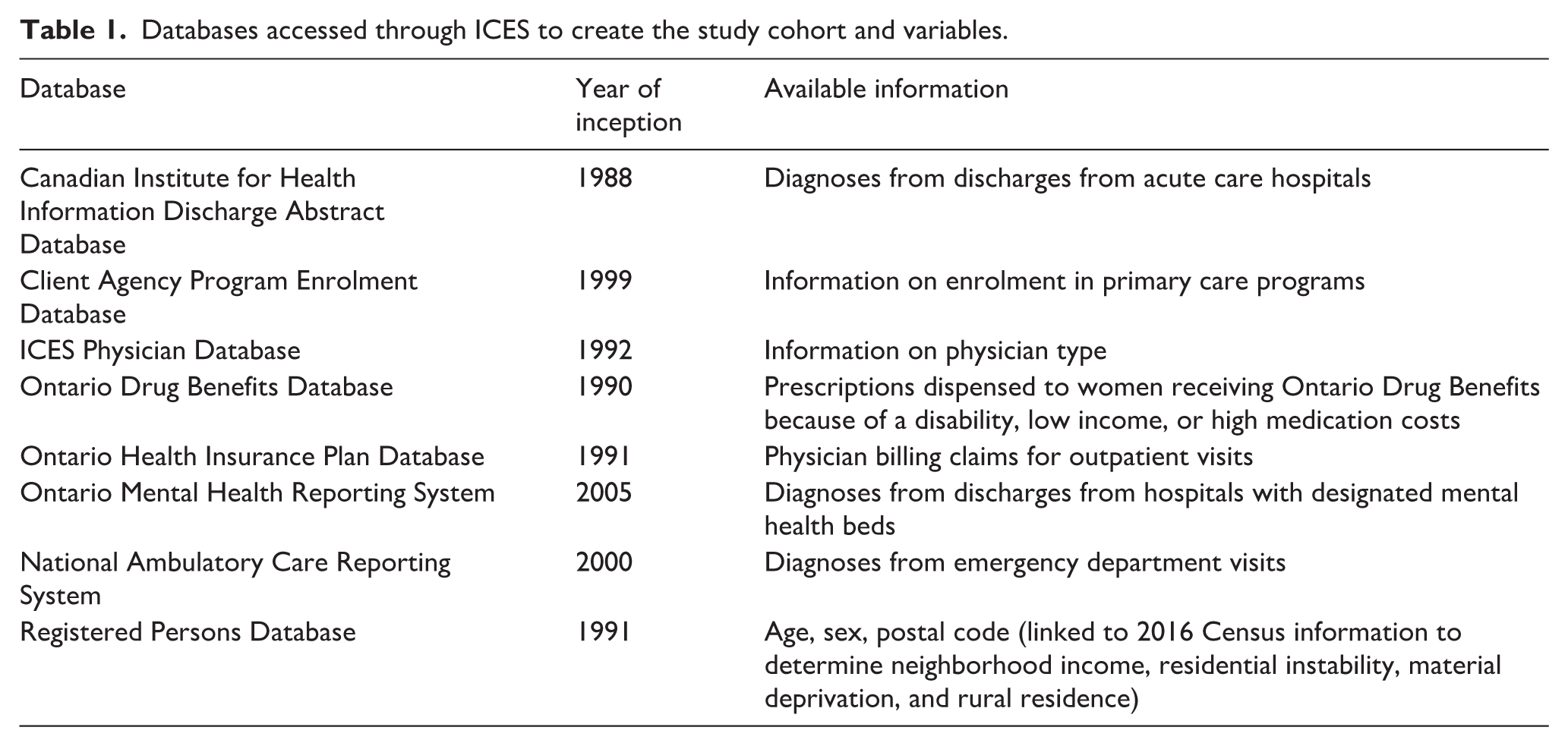
The sample for the current study was identified from administrative health data held at ICES (formerly the Institute for Clinical Evaluative Sciences), a non-profit, non-governmental organization that captures and maintains outpatient and inpatient health care data of all Ontario residents within the publicly funded health care system. We analyzed databases with diagnostic and sociodemographic information recorded during physician visits, emergency department visits, and/or hospitalizations (see Table 1). We drew prescription information from Ontario’s publicly funded medication plan. Diagnostic data in hospital databases were recorded using the Canadian Coding Standards for the International Classification of Diseases and Related Health Problems (10th revision (after 2002)) or Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV). Physician visit data were recorded using billing claim codes. In these data sets, fields for sociodemographic data, physician billing claims, and primary hospital diagnoses have been shown to be complete and accurate (Williams & Young, 1996). The data were individually linked using a unique, encoded identifier and were analyzed at the ICES facility in Toronto, Ontario.
Databases accessed through ICES to create the study cohort and variables.
Measures
Women were classified as autistic if one of the included diagnoses (see Table 2) was recorded in ⩾2 physician visits or ⩾1 emergency department visit or hospitalization from database inception to cohort entry (see Table 1 for database inception dates). Diagnoses were not necessarily made for the first time in these settings but represent opportunities where autism diagnoses could be recorded in the health record. Prior research indicates using two physician visit codes for autism or one from another source (e.g. hospitalization) has good specificity and moderate sensitivity when examining the validity of administrative health data relative to gold standard autism assessment methods (Dodds et al., 2009). The comparison group was comprised of all women without autism diagnoses.
Diagnostic codes for autism.
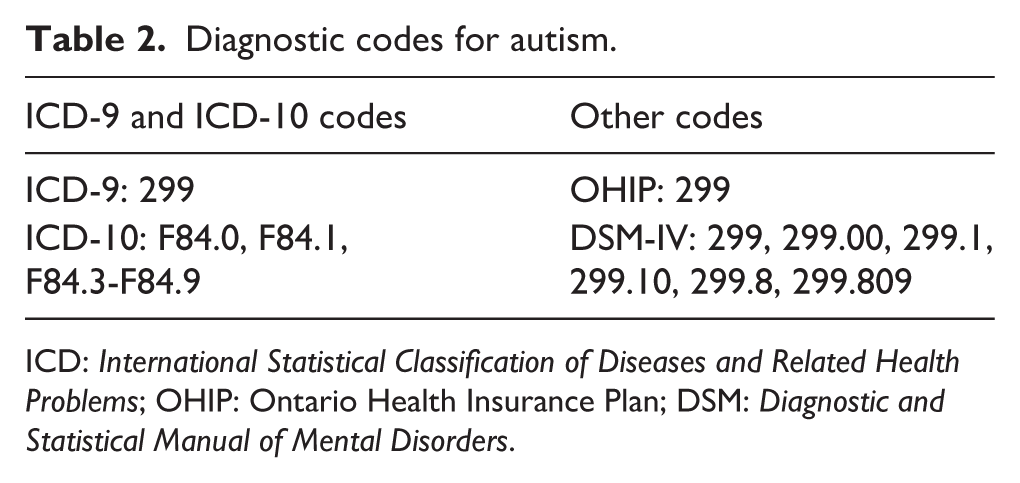
ICD: International Statistical Classification of Diseases and Related Health Problems; OHIP: Ontario Health Insurance Plan; DSM: Diagnostic and Statistical Manual of Mental Disorders.
We compared the two groups of women on age distributions and the following variables that are known to influence risks for adverse reproductive, maternal, and neonatal outcomes (World Health Organization, 2012):
Social determinants of health
Neighborhood income quintiles were derived by linking 2016 Canadian Census data on area-level median income to residential postal codes. Material deprivation and residential instability quintiles, also derived by linking Census data to postal codes, were measured using the Ontario Marginalization Index (Matheson & van Ingen, 2016) and represented area-level concentrations of individuals unable to access six indicators of basic material needs or experiencing seven indicators of housing or family instability, respectively (Supplemental Table 1). Neighborhoods were classified as either rural or urban using the Rurality Index of Ontario, which uses 10 indicators to classify neighborhoods as urban (scores of 0–44) or rural (scores of ⩾45) (Kralj, 2000) (Supplemental Table 1).
Chronic medical conditions
Validated disease registries were used to identify the presence of HIV infection (Antoniou et al., 2011) and three common chronic medical conditions among reproductive-aged women: diabetes, hypertension, and asthma (Gershon et al., 2009; Hux et al., 2002; Tu et al., 2007). More broadly, we employed the Johns Hopkins ACG ® System Version 9.0 to characterize comorbid conditions as “stable” or “unstable.” Stability was determined on the basis of condition severity and risk of complications with “unstable” conditions having greater acute health care use (Johns Hopkins Bloomberg School of Public Health, 2009).
Psychiatric conditions
Measures of mental health included psychotic mental illness, mood and anxiety disorders, substance use disorders, and other mental illness diagnosed during physician visits, emergency department visits and hospitalizations, and self-harm presenting in the emergency department, all in the 2 years before cohort entry (2015–2017; see Supplemental Table 2).
Potentially teratogenic medication use
Among those eligible for Ontario’s public drug benefits (approximately 49.1% of autistic women and 11.4% of non-autistic women), the use of potentially teratogenic medications was measured in the year before cohort entry (2016–2017; that is, anti-infectives; anti-parasitic agents; anti-epileptic agents; anti-neoplastic agents; anti-thrombotic agents; dermatological agents; immunomodulating agents; pituitary, hypothalamic, and sex hormones; psycholeptic and psychoanaleptic agents; renin angiotensin system agents; statins; and other agents; Zomerdijk et al., 2015).
Experience of assault
We measured history of assault (i.e. physical or sexual assault or other maltreatment) as recorded in emergency department visits or hospitalizations since database inception (Ray et al., 2008).
Continuity of primary care
The Usual Provider Continuity Index, which calculates the proportion of visits to all primary care providers made to the individual’s usual primary care provider in the 2-year period before cohort entry (2015–2017), was used to measure continuity of primary care (Jee & Cabana, 2006). Continuity of primary care was categorized as low (⩽50% of primary care visits made to the usual provider), moderate (51%–80%), or high (>80%). Individuals with fewer than three primary care visits in this period were characterized as infrequent users.
Analyses
Statistical analyses were performed with SAS version 9.4. Crude analyses and age-standardized analyses were conducted. Standardized differences were used to examine the clinical significance of differences between groups. Clinically meaningful standardized differences are those of at least 0.10 (Austin, 2009). Unlike p values, standardized differences are not influenced by sample sizes and are therefore more appropriate for large population-based studies (Mamdani et al., 2005).
Results
A total of 6,870 fifteen- to 44-year-old autistic women were identified. The autistic group had a greater percentage of women falling within the two youngest age categories (15–19 years and 20–24 years; 38.3% and 28.1%, respectively) and fewer autistic women were in the three oldest age categories (30–34 years, 35–39 years, and 40–44 years; 8.3%, 5.7%, and 3.7%, respectively). Table 3 describes the health characteristics of reproductive-aged autistic women and non-autistic women, without age standardization. Table 4 provides age-standardized values.
Health characteristics of 15- to 44-year-old autistic women and non-autistic women in Ontario, 2017.

Note. Bold faced values signify standardized differences of at least 0.10.
The denominator for teratogenic medication use is women receiving medications under Ontario’s publicly funded drug benefits program for autistic women (n = 3,372) and non-autistic women (n = 306,857).
Age-standardized health characteristics of 15- to 44-year-old autistic women and non-autistic women in Ontario, 2017.
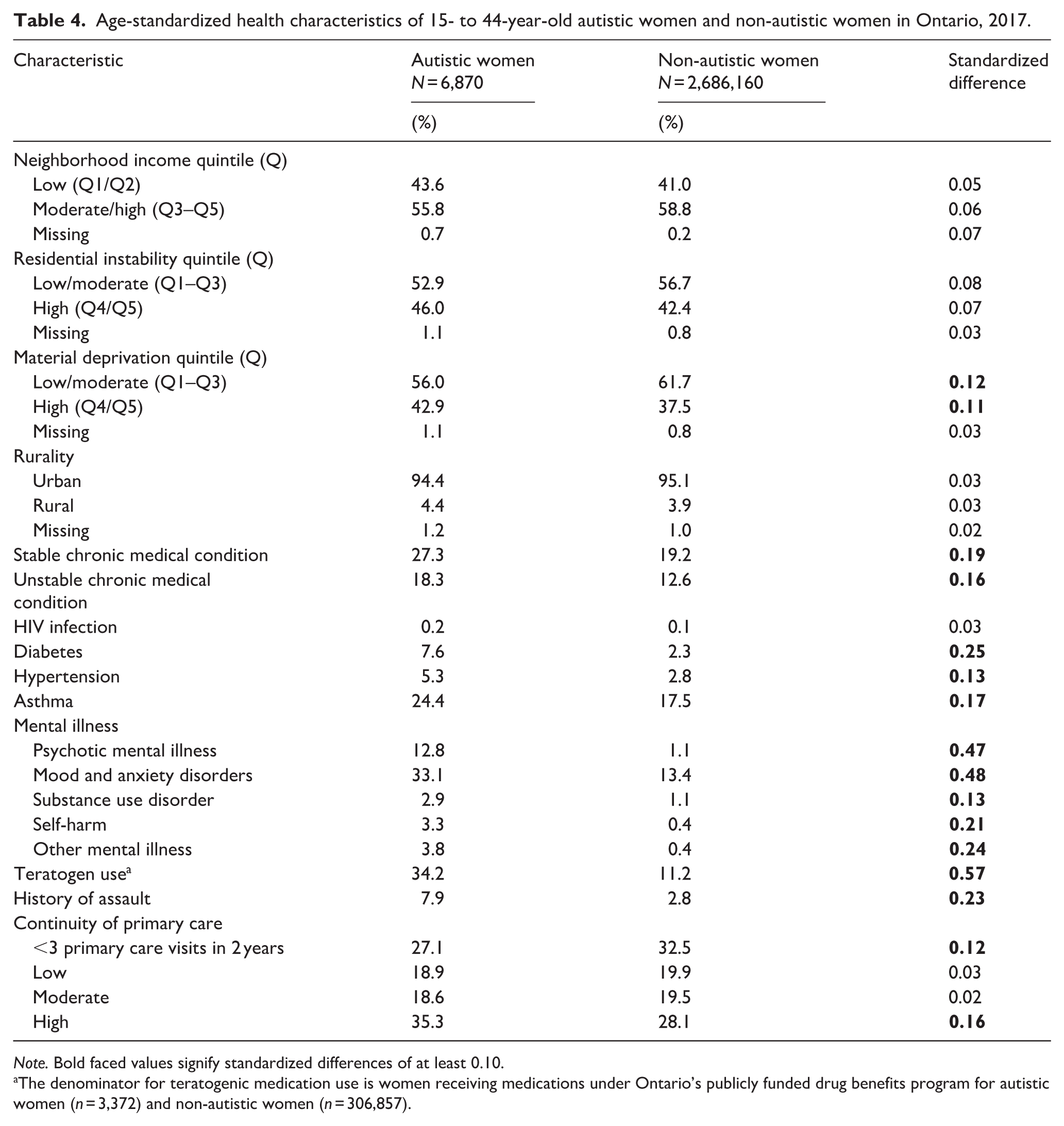
Note. Bold faced values signify standardized differences of at least 0.10. a
The denominator for teratogenic medication use is women receiving medications under Ontario’s publicly funded drug benefits program for autistic women (n = 3,372) and non-autistic women (n = 306,857).
Compared with non-autistic women, autistic women showed a similar distribution related to neighborhood income (i.e. lowest two quintiles: 42.0% vs 41.0%), residential instability (i.e. highest two quintiles: 43.3% vs 42.4%), and material deprivation (i.e. highest two quintiles: 41.7% vs 37.5%; all standardized differences < 0.10). However, after age standardization, autistic women were more likely to live in areas with high material deprivation (42.9% vs 37.5%). Autistic women were equally as likely to reside in rural regions compared with non-autistic women (4.4% vs 3.9%).
Autistic women had higher rates of diabetes (4.3% vs 2.3%) and asthma (26.2% vs 17.5%), but not hypertension or stable or unstable chronic medical conditions compared with non-autistic women. Yet, after age standardization, hypertension (5.3% vs 2.8%) and chronic medical conditions, both stable (27.3% vs 19.2%) and unstable (18.3% vs 12.6%), were also higher in autistic women. HIV infection rates were similar across both groups (both < 1%). Autistic women had higher rates of all psychiatric conditions compared with non-autistic women, including higher rates of psychotic mental illness (9.1% vs 1.1%), mood and anxiety disorders (31.8% vs 13.4%), substance use disorders (2.4% vs 1.1%), self-harm (3.9% vs 0.4%), and other mental illness (3.7% vs 0.4%). Findings related to these psychiatric conditions did not change substantially after age standardization.
A greater proportion of autistic women had used potentially teratogenic medication in the previous year (28.8%) compared with non-autistic women (11.2%). Autistic women were more likely to have experienced assault at some point in their lives (5.8%) compared with non-autistic women (2.8%). Neither of these findings changed after age standardization.
Autistic women were more likely to have high continuity of primary care (35.3%) compared with non-autistic women (28.1%), even after age standardization. Autistic women were less likely than non-autistic women to have fewer than three visits during the 2-year observation period after age standardization (27.1% vs 32.5%).
Discussion
This is the first population-based study to comprehensively describe the health characteristics of reproductive-aged autistic women compared with non-autistic women. We observed increased rates of material deprivation, chronic medical conditions, psychiatric conditions, use of potentially teratogenic medications, and history of assault among autistic women. Autistic women had better continuity of primary care than non-autistic women. Overall, reproductive-aged autistic women had poorer health compared with non-autistic women and this trend persisted after controlling for the lower average age in the autism cohort compared with non-autistic women. These findings support the idea that health interventions that appropriately meet the needs of autistic women in their childbearing years are needed.
Our results largely echo past population-based health research of autistic individuals. Our finding that autistic women were likely to live in areas with high material deprivation corroborates previous findings of elevated rates of disadvantaged housing among autistic adults in the United Kingdom (Brugha et al., 2011). Consistent with our findings, Croen and colleagues (2015) reported higher rates of chronic medical conditions (e.g. diabetes, asthma, and hypertension) and some psychiatric conditions (e.g. psychosis, anxiety) in 405 working-age U.S. autistic women, compared with an age-matched comparison group of non-autistic women. Similar to the increased rate of potentially teratogenic medication use in our sample, Zerbo and colleagues (2019) found that a significantly higher proportion of autistic adults received a prescription for psychotherapeutic and anticonvulsant medications compared with age-matched adults in the general U.S. population. The finding that autistic women were more likely to have been victims of assault in the current study also aligns with results from the Child and Adolescent Twin Study in Sweden where 18-year-old autistic girls reported an almost threefold increased risk of coercive sexual victimization compared to those without autism (Ohlsson Gotby et al., 2018). However, the results of past studies were not stratified by sex, did not focus on the reproductive years, and/or relied on self-report measures. As such, the current study presents new data, with its use of population-based administrative health data to examine a broad range of health characteristics among all women of reproductive age.
Our findings highlight significant disparities with respect to the health and well-being of reproductive-aged autistic women. Past research has focused primarily on individual-level factors that may account for such disparities. For instance, limited sexual knowledge of autistic women has been identified as a factor increasing their vulnerability to abuse (Brown-Lavoie et al., 2014; Kanfiszer et al., 2017). Solely focusing on individual challenges, however, does not appropriately speak to structural and societal factors at play, such as poverty (Mathews, 2018; Roulstone et al., 2011).
Addressing these broader socio-structural factors, autistic adults have described numerous systemic barriers preventing them from accessing effective health care (Mason et al., 2019). While it is encouraging that approximately one third of autistic women in the current study had high continuity of primary care over a 2-year period, it is important to note that continuity of primary care is only one index of health care access and may not appropriately reflect the perceived quality of care received among autistic women. Previous research has highlighted high levels of dissatisfaction among autistic adults with respect to health care (Lum et al., 2014; Nicolaidis et al., 2013; Raymaker et al., 2017), and autistic women have further described how health care providers’ lack of understanding of how autism may present in women can impede the patient–provider relationship (Tint & Weiss, 2018). Future research should incorporate more nuanced measures of health care quality. In addition, given the high rates of co-occurring medical and psychiatric conditions in the current study, it will be important to further understand how to optimize communication between health care providers to ensure appropriate care is provided for the range of care needs with which reproductive-aged autistic women may present.
To this effect, health care providers have acknowledged gaps in education and training about autism, as well as time constraints and service reimbursement issues related to time spent providing care for autistic adults (Bruder et al., 2012; Warfield et al., 2015). Encouragingly, recent work has demonstrated ways to address these difficulties and build the capacity of health care providers to effectively address the needs of autistic individuals, especially in the areas of mental health and primary care (Maddox et al., 2019; Maddox & Gaus, 2019; Mazurek et al., 2017; Sohl et al., 2017). Recognizing the historically male-dominated and child-focused views of autism research and service delivery to date (Edwards et al., 2012; Kirkovski et al., 2013; Kreiser & White, 2014; Watkins et al., 2014), it will be important for future clinician training efforts to include discussion of the health needs of reproductive-aged autistic women. Specifically, it is important to raise the awareness of clinicians providing women’s health care (e.g. primary care physicians, obstetricians, and gynecologists) of the care needs of their autistic patients (Kassee et al., 2020).
Our findings underscore important target areas for health interventions for reproductive-aged autistic women. For instance, while decision aids for psychotropic medication use in pregnancy have been designed for women with depression in the general population who are planning a pregnancy (Vigod et al., 2019), we do not know whether these tools are beneficial for autistic women. It is essential to tailor health interventions to the specific needs of different populations (Mitra et al., 2015; Ruhl & Moran, 2008) and it is likely that modifications to existing interventions would be needed to adequately address the unique needs of autistic women (e.g. structured information, enhanced visual supports and social stories to account for social communication differences, and attention to sensory challenges). In addition, although established health promotion programs exist for women with intellectual and developmental disabilities (e.g. Lunsky et al., 2003), we do not know how often these programs are offered to and accessed by autistic women. Further study on implementation efforts is needed.
Strengths of the current study include the use of population-based administrative health data to create a large and generalizable cohort of reproductive-aged autistic women, which adds to the limited research on the overall health of this understudied population. However, this study has limitations. Our use of administrative data may be subject to misclassification bias and some women identified as autistic in our sample may be false positives. Autistic women in our sample may also have been misidentified as non-autistic if they did not have a health care encounter with a relevant diagnostic code. If this is the case, the findings are conservatively biased and the differences observed here may be greater in the population. In addition, autism tends to be underdiagnosed in girls and women (Loomes et al., 2017). Associated misclassification errors in our sample, if present, would bias the results toward the null. It is also important to note that outpatient billing in Ontario only allows for a single billing code per health care visit. As such, any observed differences between autistic women and the comparison group of non-autistic women could be due to other factors not measured herein. For example, the autistic women in our cohort could have co-occurring disabilities (e.g. intellectual disabilities) that could explain some of our results. Moreover, autistic women in our cohort differed significantly in age from the women in the comparison group. While our statistical analyses controlled for such a difference, it will be helpful for future studies to include an age-matched comparison group. In addition, we did not study important health conditions (e.g. epilepsy, gastrointestinal symptoms, sleep difficulties) commonly associated with autism and other characteristics relevant to reproductive-aged health such as smoking or body mass index. We were also limited to area-level data to measure the social determinants of health. Finally, while race and ethnicity have been associated with health characteristics among the general population (Denny et al., 2012; Hawks et al., 2018), such information is not collected in Ontario health records and thus could not be included in our study. These remain important areas for future research.
Conclusion
Autistic women’s health has received inadequate attention to date (Sulpizi, 1996; Tint et al., 2018). Considering the significant disparities in the health of reproductive-aged autistic women in the current study, explicit inclusion of this population’s health needs is required within patient education materials, as well as the education and training of health care professionals. Further research is needed to direct these efforts and the development of autism-sensitive best practices.
Supplemental Material
sj-pdf-1-aut-10.1177_1362361320982819 – Supplemental material for Health characteristics of reproductive-aged autistic women in Ontario: A population-based, cross-sectional study
Supplemental material, sj-pdf-1-aut-10.1177_1362361320982819 for Health characteristics of reproductive-aged autistic women in Ontario: A population-based, cross-sectional study by Ami Tint, Hilary K Brown, Simon Chen, Meng-Chuan Lai, Lesley A Tarasoff, Simone N Vigod, Susan Parish, Susan M Havercamp and Yona Lunsky in Autism
Footnotes
Disclaimer
Parts of this material are based on data and information compiled and provided by the Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions, and statements expressed herein are those of the author, and not necessarily those of CIHI.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author was supported by a Canadian Institutes of Health Research Postdoctoral Fellowship. Research reported in this publication was supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health (Award No. 5R01HD092326). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. This study was also supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). The opinions, results, and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES or the MOHLTC is intended or should be inferred. The funding source had no role in the study design, data collection, analysis, data interpretation, report writing, or decision to submit the article for publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.