
Abstract
This study examined objective quality of life (work, academic success, living situation, relationships, support system) and subjective quality of life (Sense of Coherence and Short-Form Health Survey-36) in an adult sample of males (n = 50, mean age: 30 years) with Asperger syndrome diagnosed in childhood and followed prospectively over two decades. The association between long-term diagnostic stability of an autism spectrum disorder and/or comorbid psychiatric disorders with quality of life was also examined. The results showed great variability as regards quality of life. The subsample that no longer fulfilled an autism spectrum disorder had full-time jobs or studies (10/11), independent living (100%), and reported having two or more friends (100%). In the stable autism spectrum disorder group, 41% had full-time job or studies, 51% lived independently, and 33% reported two or more friends, and a significant minority had specialized employments, lived with support from the government, or had no friends. Academic success was positively correlated with IQ. A majority of the total group scored average Sense of Coherence scores, and the mean for Short-Form Health Survey-36 was above average regarding psychical health and below average regarding mental health. Stability of autism spectrum disorder diagnosis was associated with objective but not subjective quality of life, while psychiatric comorbidity was associated with subjective but not objective quality of life.
Introduction
When examining general “outcome” in any clinical population, the concept of quality of life (QoL) should always be considered. QoL has been defined as “personal well-being or satisfaction with life, as well as physical and material well-being, relations with other people, social, communal, civic activities, personal development and fulfilment, positive mental health, a degree of goodness, and is related to health” (Eriksson and Lindström, 2007: 939). This means that when QoL is assessed, one has to take the individuals’ subjective feelings about their life (subjective QoL), as well as their de facto psychosocial life situation, that is, living situation, occupation, relationships, and so on (objective QoL), into account.
Asperger syndrome (AS) is an autism spectrum disorder (ASD) that is characterized by difficulties in social functioning, repetitive behaviors, and/or interests and usually features communicative difficulties in the context of normal range IQ (American Psychiatric Association (APA), 1994; Gillberg and Gillberg, 1989). Hans Asperger (1944) himself described in his original article account of AS (at the time known as autistic psychopathy) that individuals with AS often functioned quite well regarding certain aspects of objective QoL, for example academics and work. This, he claimed, was especially true if their intelligence was high and they had special interests that were useful, such as mathematics, but he also emphasised that they still had difficulties regarding social life in general. In the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) and 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10; World Health Organization (WHO), 1992), AS was a specific diagnosis within the ASD construct, but in the new Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013) the specific AS diagnosis has been removed and now there is only the diagnosis of ASD.
Studies on the objective QoL of AS and other ASDs with normal range IQ report varied results ranging from well-adjusted members of society to individuals who lead lives isolated from society and have little to no autonomy (Balfe and Tantam, 2010; Barneveld et al., 2014; Cederlund et al., 2008; Eaves and Ho, 2008; Engstrom et al., 2003; Howlin et al., 2004, 2013). There are no clear cut indicators of why objective QoL varies to this extent, but factors such as degree of support, intelligence, ASD symptom severity, early language development, specific type of ASD diagnosis, and psychiatric comorbidity have been shown to affect objective QoL.
The subjective aspects of QoL in adults with ASD have been thoroughly examined. In a meta-analysis of QoL in relation to ASD (Van Heijst and Geurts, 2015), there was strong evidence that individuals with ASD have significantly worse subjective QoL than controls. There are several ways to measure subjective QoL and among them are those related to the concepts of Sense of Coherence (SoC) and Health-Related QoL (HRQoL).
SoC was developed according to Antonovsky’s (1979) salutogenic model which postulates that SoC is needed in order to successfully cope with stressors and thus promote health. SoC has been shown to affect different aspects of the individual’s well-being and is closely related to subjective QoL (Eriksson and Lindström, 2007). Studies on SoC have shown that low SoC is associated with—among many negative aspects—poor mental health (Mattisson et al., 2014). Studies of SoC in relation to ASD have mostly focused on the parents of individuals with ASD and very little is known regarding SoC in individuals who themselves have an ASD. There have been a few treatment studies (Hesselmark et al., 2014; Wentz et al., 2012) where SoC has been used as a treatment outcome measure in clinical populations with ASD. In these studies, the treatment group has shown low SoC at baseline.
HRQoL is a multi-dimensional measure of the individual’s perception regarding various aspects of mental/emotional and physical health and well-being, as well as relationships and participation in society. HRQoL is exclusively focused on health and because of this has a more narrow focus within the concept of subjective QoL. Individuals with ASD have been found to have lower ratings on HRQoL measures than healthy controls (Kamp-Becker et al., 2010; Lin, 2014) but to have higher ratings than patients with schizophrenia. It has also been shown that HRQoL measures are associated with psychiatric comorbidity, daily living skills, and social relationships in individuals with ASD (Kamp-Becker et al., 2010; Lin, 2014).
Individuals with AS/ASD with average range IQ have repeatedly been shown to be at high risk for other psychiatric disorders (Gillberg et al., 2016; Lugnegård et al., 2011; Roy et al., 2015). It has been suggested (Gillberg and Fernell, 2014) that individuals with ASD and no psychiatric comorbidity function fairly well in life, and that only when an ASD is combined with another psychiatric, developmental, or physical disorder (aka ASD plus), you can expect severe difficulties in life. In a study by Mazzone et al. (2013), a connection between depressive symptoms and global functioning in an AS/ASD sample was found.
The concept of optimal outcome in ASD (i.e. the type of outcome represented by individuals who at follow-up no longer fulfill criteria for ASD and who function quite well) has come into focus (Fein et al., 2013) during the last few years as more and more studies have shown that a subsample of individuals with ASD will not meet criteria for a diagnosis of ASD at follow-up (Helles et al., 2015; Woolfenden et al., 2012). To our knowledge, no studies have been published that contrast optimal outcome/diagnostic stability in ASD with corresponding QoL.
Here, we report on a second follow-up study (at mean age 30 years) of a clinical cohort of men with AS diagnosed in childhood and followed prospectively over two decades (the first follow-up was made at mean age of 20 years). The aim of this study was to assess the objective QoL (i.e. work, living situation, relationships, and support system) and subjective QoL in an adult sample of males with AS diagnosed in childhood and followed over 20 years. A secondary aim was to assess whether long-term diagnostic stability of an ASD and/or comorbid psychiatric disorders were related to the different aspects of QoL. A third aim was to establish whether or not there is a relationship between objective and subjective measures of QoL in this cohort.
Methods
Procedure
A group of 100 males with AS has been followed since their original diagnosis in childhood. They have been thoroughly assessed and have been found to be representative of all males diagnosed with AS in Gothenburg during the 1980s and 1990s (Cederlund and Gillberg, 2004; Gillberg and Cederlund, 2005). Initially, there was a plan to also include 30 females, but only 7 cases were found to meet the inclusion criteria during the 15-year period covered, so due to lack of statistical power, females were excluded.
The inclusion criteria were as follows: (1) all consecutive cases with a registered clinical diagnosis of AS according to the Gillberg criteria (Gillberg and Gillberg, 1989) at the Child Neuropsychiatric Clinic in Gothenburg between 1985 and 1999, (2) Full-Scale IQ (FSIQ) >70 at the time of diagnosis (T0), and (3) age > 16 years at first follow-up (T1) in 2002–2003.
Of the 100 individuals, 76 agreed to participate at T1 (Cederlund et al., 2008) and 50 agreed to participate at the second follow-up (T2), 47 of whom participated at both T1 and T2. In the T2 study, performed in 2011–2013, the original selection group was contacted again by letter with information about the study and then contacted by telephone and asked to participate. Of the individuals, 7 were not contacted because they had previously declared no interest in participating, 1 had died since T1, 35 declined to participate in the study, and 7 were unreachable by phone or mail, that is, 50 individuals participated at T2.
The research team comprised a psychiatrist and a clinical psychologist, both with extensive experience in the field of ASD and other developmental disorders. Data were mostly collected during a 4–6 h visit to the Gillberg Neuropsychiatry Centre (n = 46), but one participant was assessed at home, two were interviewed over the phone as were their parents, and one participant did not agree to be interviewed himself but allowed us to interview his parents. The two participants interviewed by phone had moved far away from the region and were not able to travel to the clinic for assessment. The individuals interviewed over the phone were sent the survey forms by mail and sent their answers back to the clinic.
To ensure that participants understood the questions in the self-administered tests, the psychologist was always close by to answer any questions and the participants were encouraged to ask whether there were something they did not understand.
Participants
A thorough analysis of attrition and project design is presented in Helles et al. (2015) and Gillberg et al. (2016). The participants at T2 differed from non-participants regarding FSIQ and Performance IQ at T1 and Performance IQ at T0, with the participants at T2 having a significantly higher score on these measures than those not participating at T2. However, participants and non-participants did not differ regarding ASD symptom severity at T0 (measured with the Autism Spectrum Screening Questionnaire (ASSQ) (Ehlers et al., 1999)) or T1 (measured with the Autism Spectrum Diagnostic Interview (ASDI) (Gillberg et al., 2001)), attention deficit and hyperactivity symptoms at T1 (measured by the Swanson, Nolan and Pelham Questionnaire (4th ed.; Swanson, 1992), depressive symptoms at T1 (measured by the Beck Depression Inventory; Beck and Steer (1996)), general functioning at T1 (defined by Global Assessment of Functioning (APA, 1994)), or overall outcome (defined by Lotter’s (1978) outcome criteria (Gillberg and Steffenburg, 1987) looking at social life and functioning at school or work) at T1.
Of the 50 participants, 11 in the study no longer met criteria for an ASD diagnosis according to the DSM-IV (APA, 1994). Diagnostic assessment was based on ASDI and clinical assessment, and non-diagnosis was, in most cases, confirmed using the Diagnostic Interview of Social and Communicative Disorders (Wing et al., 2002) with a parent (Helles et al., 2015). These 11 males had all met criteria for AS according to Gillberg and Gillberg criteria in childhood (a diagnosis closely related to ICD-10 Autistic disorder (Leekam et al., 2000)) and, in most cases (8 out of 11), also met criteria for a DSM-IV ASD diagnosis in young adult life at T1 (Cederlund et al., 2008). This subgroup will further on be referred to as the No longer ASD group.
Results regarding current psychiatric comorbidity in the cohort have been presented in Gillberg et al. (2016). Psychiatric disorders assessed were depressive disorders (depression and dysthymia), anxiety disorders (post-traumatic stress disorder, panic disorder, social phobia, and general anxiety disorder), attention-deficit hyperactivity disorder (ADHD), obsessive–compulsive disorder (OCD), bipolar disorder, psychotic disorders, and alcohol and drug dependency. None had current psychosis, bipolar disorder, drug dependency, post-traumatic stress disorder, or dysthymia, but 24 out of the 39 individuals who still met criteria for ASD diagnosis at T2 also met criteria for at least one other psychiatric disorder. Current psychiatric disorders confirmed were ADHD (n = 14), mood disorder (n = 14), anxiety disorder (n = 8), OCD (n = 4), and alcohol dependency (n = 2). The group of 15 who only met criteria for ASD but with no comorbidity will henceforth be referred to as ASD only and the 24 with comorbidity will be referred to as ASD plus. Of the 11 individuals in the No longer ASD group, 3 also had psychiatric comorbidity (1 with ADHD and 2 with depression). They are included in the No longer ASD group.
The three subgroups are presented in Table 1. There were no significant differences regarding age at T0 or T2, FSIQ at T0 (measured with Wechsler Intelligence Scale for Children (3rd ed.; WISC-III; Wechsler, 1991, 2002)) or T2 (measured with Wechsler Adult Intelligence Scale, 3rd ed. (WAIS-III)), or degree of autism spectrum symptoms at T0 ASSQ (Ehlers et al., 1999)). There were, as would be suspected, significant differences between the No longer ASD group and both the ASD only and ASD plus groups regarding degree of autism spectrum symptoms at T2 (measured with the ASDI (Gillberg et al., 2001)), but not between the ASD only and ASD plus groups regarding this measure (Table 1).
Comparison of background variables between No longer ASD, ASD only, and ASD plus groups.
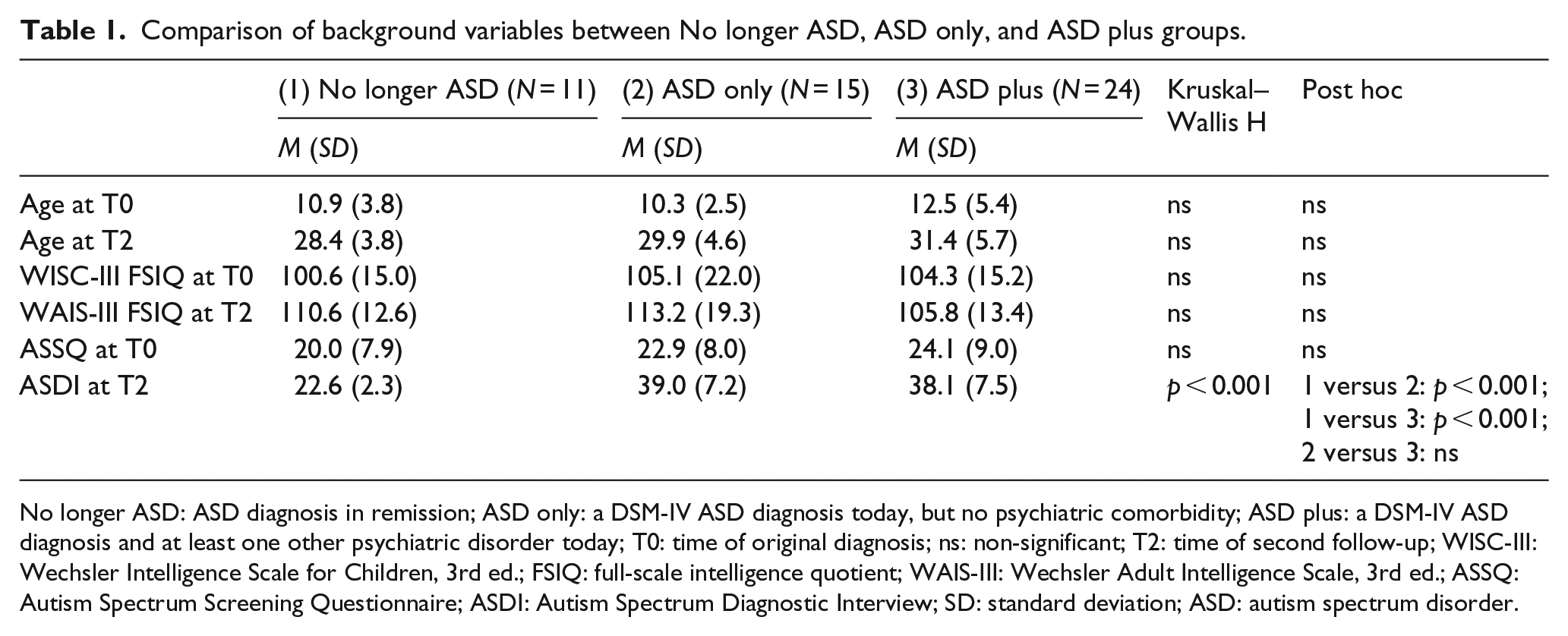
No longer ASD: ASD diagnosis in remission; ASD only: a DSM-IV ASD diagnosis today, but no psychiatric comorbidity; ASD plus: a DSM-IV ASD diagnosis and at least one other psychiatric disorder today; T0: time of original diagnosis; ns: non-significant; T2: time of second follow-up; WISC-III: Wechsler Intelligence Scale for Children, 3rd ed.; FSIQ: full-scale intelligence quotient; WAIS-III: Wechsler Adult Intelligence Scale, 3rd ed.; ASSQ: Autism Spectrum Screening Questionnaire; ASDI: Autism Spectrum Diagnostic Interview; SD: standard deviation; ASD: autism spectrum disorder.
Ethics
Ethical approval was obtained from the Regional Ethical Approval Board in Gothenburg (reference: 508-10). All participants signed an informed consent form. Information regarding the study was given both orally and in writing, and all participants were asked whether they needed any further explanations before signing the consent form.
Measures
Objective QoL
Psychosocial interview form
Information regarding objective QoL was collected using a structured interview form that covered friendship (how many friends did they have, defined as a person they considered a friend but who was not a sibling, romantic partner, parent, or personal assistant), romantic relationships (if they were married, lived with a partner, had a girl-/boyfriend, or if they ever had experienced a romantic relationship), occupation (if they were employed or not, and if they were employed did they have a regular employment, a wage-subsided employment, or a specialized employment), educational history (did they have a high school degree, did they have a college/university degree, did they currently study at college/university, and had they dropped out of college/university without taking a degree), and living situation (did they live with parents, live alone, at a group home, and did they have support from the municipality). A similar interview form was used in the Cederlund et al.’s (2008) study.
Subjective QoL
Medical outcome study Short-Form Health Survey version 2.0 (
Statistical analysis
All data analyses were made with IBM SPSS Statistics for Windows, Version 22.0 (IBM Corp, Armonk, NY, USA). Non-parametric statistics was used in most calculations, and all significance tests were two-tailed. Significance level was set at p = 0.01, in part because of the fairly large number of calculations made and in part to enhance comparability with other longitudinal studies (i.e. Howlin et al., 2004, 2013), while also maintaining a balance between type-I and type-II errors. With a view to increase comparability/readability, means are presented even in cases where the statistical analysis was made based on medians or ranks and percentages are presented even in cases where the statistical analysis was made based on medians or ranks. Factors regarding objective QoL were ranked on an ordinal scale in the order presented in Table 2. Group comparison between the No longer ASD, ASD only, and ASD plus groups was made with the Kruskal–Wallis H test, and post hoc analysis was made with the Mann–Whitney U test. Physical component summary (PCS) and mental component summary (MCS) scores on the SF-36v2 were compared with the norm mean of 50 using a one-sample t-test. Spearman’s rho was used to assess correlations between ASDI total score and WAIS-III FSIQ with objective QoL factors ranked on an ordinal scale in the order presented in Table 2. Linear regression models were used to assess whether objective QoL affects subjective QoL, as well as assessing the effect of ASD diagnostic stability and psychiatric comorbidity, while also controlling for intelligence and age. Due to the small sample size and limited power of the regression model, five theoretically important measures were chosen (friendship, living situation, occupation, comorbidity, and ASD diagnostic stability). Friendship, occupation, and living situation were ranked on the ordinal scale presented in Table 2 with higher scores indicating better functioning, psychiatric comorbidity was defined on a nominal scale either fulfilling at least one other psychiatric disorder or not, and ASD diagnostic stability was also defined on a nominal scale still either fulfilling a ASD diagnosis or not. We controlled for age and WAIS-III FSIQ (in five cases, there were no WAIS-III scores from T2 and instead, the WAIS-III scores from T1 were used). Standardized beta-coefficients are presented to enhance comparability. The same model was used assessing SoC total score, MCS score, and PCS score on the SF-36v2. SoC total score was normally distributed and was used in a linear regression model without adjustment. MCS was skewed and instead the gamma logarithm of the scores was used as this operation made normally distributed scores. PCS was fairly normally distributed and was used in a linear regression model without adjustment.
Psychosocial life situation in comparison between No longer ASD, ASD plus, and ASD only.
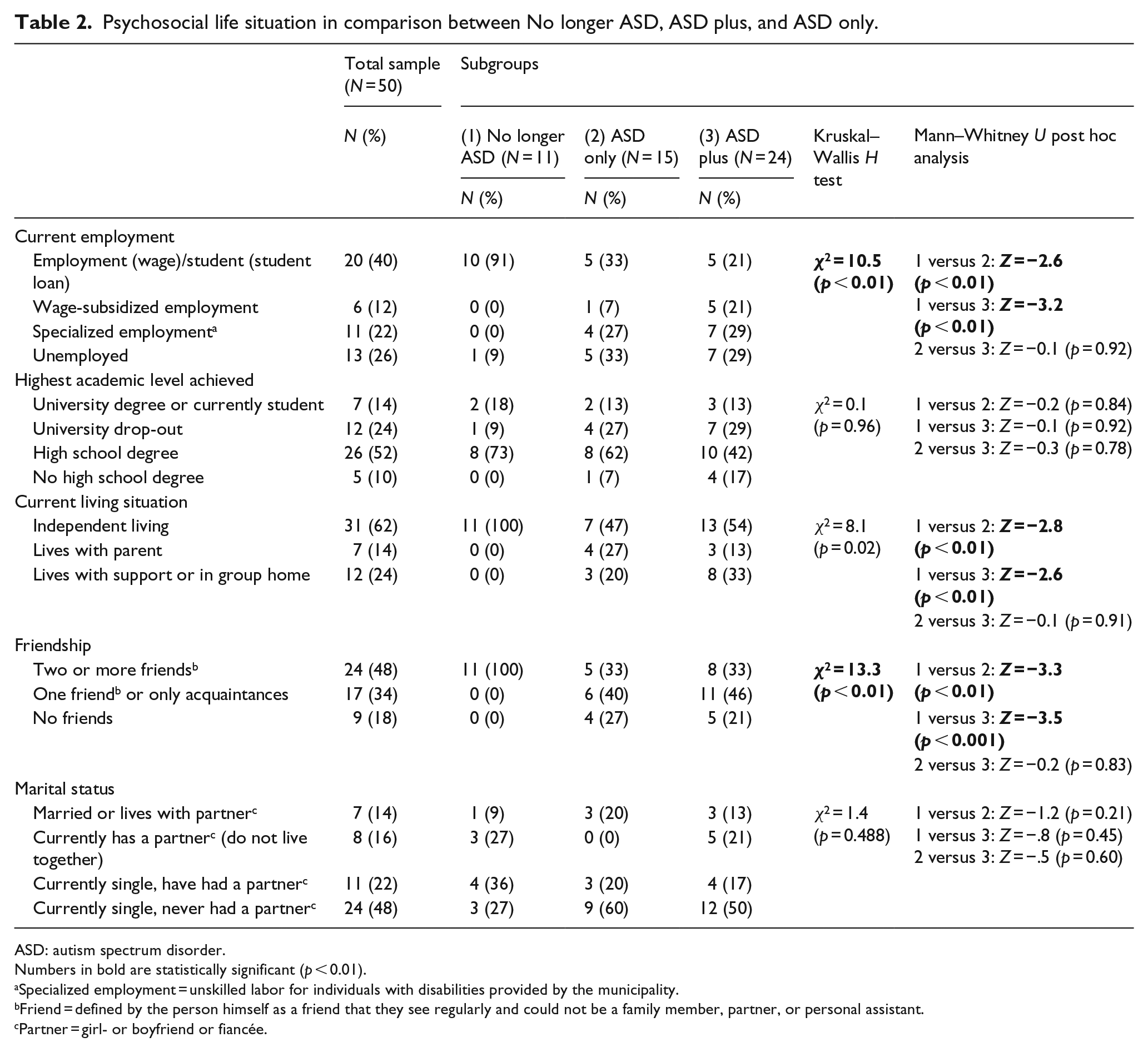
ASD: autism spectrum disorder.
Numbers in bold are statistically significant (p < 0.01).
Specialized employment = unskilled labor for individuals with disabilities provided by the municipality.
Friend = defined by the person himself as a friend that they see regularly and could not be a family member, partner, or personal assistant.
Partner = girl- or boyfriend or fiancée.
Results
Objective QoL
Employment/studies
In the entire sample, 52% had some kind of full-time job or studied full-time at university either with normal wage/student compensation (10/11 in the No longer ASD group, 33% in the ASD only group, and 21% in the ASD plus group) or with a wage-subsidized employment, that is, the government pays parts of or all of the wages, but the job is a full-time employment (7% in the ASD only group and 21% in the ASD plus group). Another 22% had a special employment from the municipality, usually unskilled labor with differing degrees of support, in Sweden known as daily activities (27% in the ASD only group and 29% in the ASD plus group), and 26% were unemployed (1/11 in the No longer ASD group, 33% in the ASD only group and 29% in the ASD plus group). The ASD plus and ASD only groups had significantly lower scores regarding independent employment than the No longer ASD group (Table 2).
Educational background
In the group, 38% were studying or had studied at university, but more than half of those who had studied at university dropped out without a university degree. There were no significant differences between the three subgroups regarding academic background (Table 2).
Living situation
Of the total study group, 62% lived independently with no organized support, albeit some were living with their partner and a few were sharing an apartment with a friend; 14% still lived at home and 24% lived in some form of supported living (most of whom were living in their own apartment with some support regarding daily care but some lived in a group home). The No longer ASD group had significantly higher scores regarding independent living than the ASD only and ASD plus groups (Table 2). On average, the No longer ASD group moved away from home at the age of 20.6 years (standard deviation (SD) = 1.4 years, median = 20.5 years), the ASD only group moved away from home at the age of 21.8 years (SD = 3.0 years, median = 21 years), with three participants still living at home at the time of the study, and the ASD plus group moved away from home at the age of 22.8 years (SD = 4.6 years, median = 22 years), with two participants still living at home. The between-group differences are non-significant.
Relationships
Regarding friendship, 48% of the total sample reported having two or more friends that they see regularly and consider as true friends (all of the No longer ASD group had two or more friends and one-third of the ASD only and ASD plus groups had two or more friends), 34% had only one friend or only acquaintances whom they did not consider as friends, while 24% of the total sample had no one that they considered as a friend or even as an acquaintance they see from time to time; 14% were married or lived with a partner and 16% had a partner whom they did not live with. Of the total sample, 22% were currently single, but had been in some kind of romantic relationship previously and 48% had never been in any kind of romantic relationship. There were no significant differences between the subgroups regarding marital status, but there were significant differences regarding friendship with the No longer ASD group having higher scores than the ASD only and ASD plus groups (Table 2).
Relationship between objective QoL and intelligence and ASD symptom load
Correlation analyses between WAIS-III FSIQ scores and objective QoL showed a significant positive correlation between academic success and intelligence (rho = 0.58, p < 0.01), but there were no significant correlation with the other QoL factors. Conversely, there was no significant correlation between ASDI scores and academic success, but significant negative correlations between ASDI scores and all other objective QoL factors were found (Table 3).
Spearman’s rho correlation between FSIQ and ASDI Total scores and objective QoL factors ranked on an ordinal scale in the order presented in Table 2.
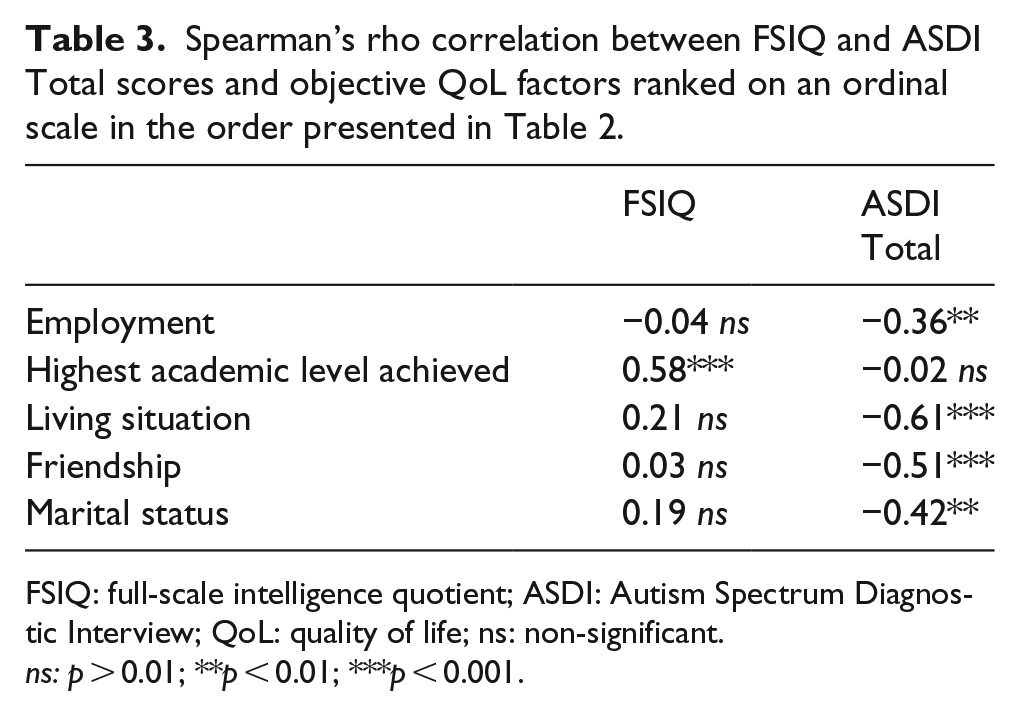
FSIQ: full-scale intelligence quotient; ASDI: Autism Spectrum Diagnostic Interview; QoL: quality of life; ns: non-significant.
ns: p > 0.01; **p < 0.01; ***p < 0.001.
Subjective QoL
SoC
The mean total SoC score for the total study group was 129.0 (SD = 22.2) in the average range for the SoC (although in the lower average range). In total, 14 participants (28%) had SoC scores below 120, indicating low SoC (13 out of 14 were from the ASD plus group), and 6 participants (12%) had SoC scores above 160, indicating high SoC (5 out of 6 were from the No longer ASD group). The ASD plus group had significantly lower Total scores and Manageability scores on the SoC when compared to the No longer ASD and ASD only groups. They also scored significantly lower on the Comprehensibility score than the No longer ASD group. There were no significant differences between the No longer ASD and ASD only groups on the SoC (Table 4).
Comparison between the No longer ASD, the ASD only and ASD plus groups in relation to Sense of Coherence.

SD: standard deviation; ASD: autism spectrum disorder; ADHD: attention-deficit hyperactivity disorder; OCD: obsessive–compulsive disorder.
Numbers in bold are statistically significant.
ASD without comorbidity.
ASD in combination with depression, ADHD, any anxiety disorder, OCD, and/or alcohol dependency.
The linear regression for SoC Total score yielded a total model with an adjusted R2 = 0.42 (p < 0.001). The regression model showed significant results regarding current psychiatric comorbidity (β = −0.50, p < 0.001). The regression model yielded non-significant results for friendship (β = 0.32, p = 0.03), ASD diagnostic stability (β = −0.13, p = 0.43), current living situation (β = 0.06, p = 0.68), and current employment status (β = 0.02, p = 0.89). Controlling for age and FSIQ showed that these factors did not add to the model while maintaining the same significance results.
SF-36v2
The total sample showed mean Physical Composite Scores (PCS) on the SF-36v2 above average compared to norm data (M = 54.3, SD = 6.3, t = 4.6, p < 0.001) and mean Mental Composite Score (MCS) below average compared to norm data (M = 42.0, SD = 9.8, t = −5.5, p < 0.001) (Table 4). There were no significant differences between the subgroups regarding PCS or MCS. There were no significant differences between the No longer ASD and ASD only groups regarding any of the subscales on the SF-36v2, but the ASD plus group scored significantly lower than the No longer ASD group regarding mental health and significantly lower than the ASD only group regarding Role-Physical, General Health, Social Functioning, and Mental Health (Table 5).
Comparison between the No longer ASD, the ASD only, and ASD plus groups in relation to Short-Form Health Survey.
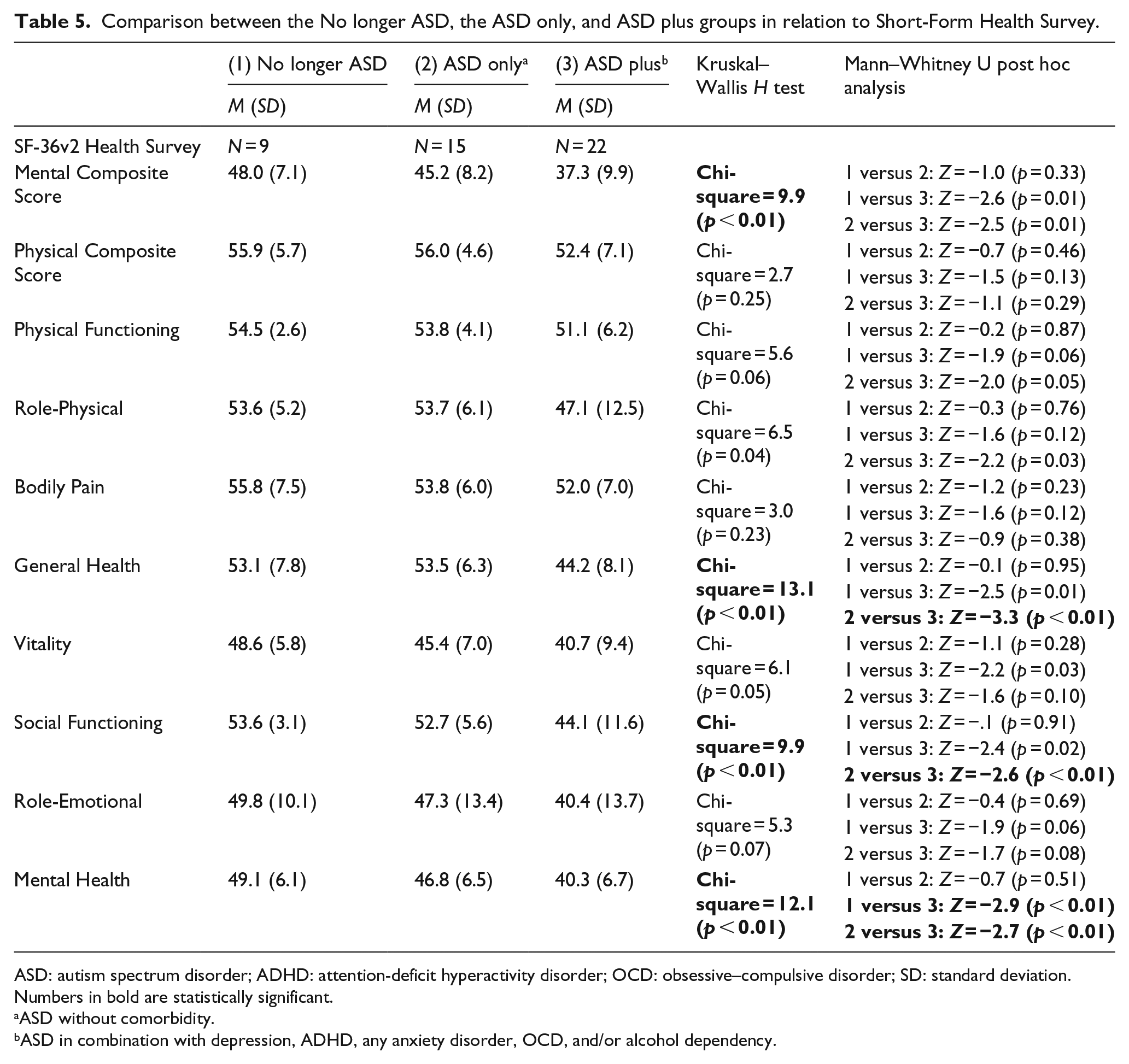
ASD: autism spectrum disorder; ADHD: attention-deficit hyperactivity disorder; OCD: obsessive–compulsive disorder; SD: standard deviation.
Numbers in bold are statistically significant.
ASD without comorbidity.
ASD in combination with depression, ADHD, any anxiety disorder, OCD, and/or alcohol dependency.
The linear regression for the PCS (adjusted R2 = 0.07, p = 0.15) yielded non-significant results. The linear regression model for MCS was significant (adjusted R2 = 0.22, p < 0.01), but none of the individual factors in the model, psychiatric comorbidity (β = −0.36, p = 0.01), current employment status (β = −0.36, p = 0.04), current living situation (β = 0.20, p = 0.20), ASD diagnostic stability (β = −0.10, p = 0.58), or friendship (β = −.07, p = 0.66), were significant at the significance level of p < 0.01.
Discussion
We found a very considerable degree of variability as regards to both objective (i.e. work, living situation, education, and relationships) and subjective (measured by the SoC and SF-36v2) QoL in a sample of males diagnosed with AS in childhood and followed over almost of two decades. Almost all of the males who no longer fulfilled criteria for an ASD had full-time jobs or studies (91% or 10/11), lived independently (100%), and reported having two or more friends (100%). Participants with a stable ASD (regardless if they had current psychiatric comorbidity or not) had much lower rates regarding these factors (about 41% had a job or studies, although many had a wage-subsidized employment, about half lived independently and about a third reported having two or more friends). About half of the individuals with a stable ASD had either a specialized employment (unskilled labor provided by the municipality) or had no job at all, about half lived either at home or with high support from the government, close to half reported having only one friend or only acquaintances, and about a quarter reported having no friends or even acquaintances. Almost half of the total group (48%) had never been in a romantic relationship (27% or 3/11 No longer ASD; 60% ASD only; 50% ASD plus), whereas a minority (30%) were currently in such a relationship. More than a third of the total group had attended or were currently attending university (27% or 3/11 No longer ASD, 40% ASD only, and 42% ASD plus), but more than half of this group (63%) had dropped out without a degree.
These results are mostly better than results from other studies. Eaves and Ho (2008) reported that 4% were fully employed with wage, 8% lived independently, and 33% had at least one friend. Balfe and Tantam (2010) reported that 28% were employed and 14% lived independently. Howlin et al. (2013) reported that 13% lived independently, 28% were employed, and 24% had one or more friends. Results from the Roy et al.’s (2015) study showed similar results as this study regarding employment (46%), romantic relationships (28%), and independent living (70%).
Compared to general population data from the Statistics Sweden (SCB), there are some similarities and differences between the males in our study compared to the average Swedish adult male. In January 2012, about 74% of males in the age of 25–34 years were employed (including wage-subsidized employment but excluding students and specialized employments) (Statistics Sweden, 2012). This is compared to our sample where 73% of those who no longer fulfilled an ASD and 36% of those with a stable ASD were employed. In Sweden, about 41% of men between the ages of 25 and 34 years have studied or studies at university (Statistics Sweden, 2015a) and about 12% of men drop out without a degree (Statistics Sweden, 2014), compared to our sample where 27% in the No longer ASD group and 39% of the males with a stable ASD had studied at university and one out of three individuals in the No longer ASD group and 69% in the stable ASD group had dropped out without a degree. Men in Sweden move away from home at a median age of 21.8 years (Statistics Sweden, 2015b), while the median age for the males who no longer fulfilled an ASD was 20.5 years and for the males with a stable ASD was 22 years (excluding those still living at home). All in all, these comparisons show that the No longer ASD group is fairly similar to the national average, while those with a stable ASD do study at university and move from home at the national average but they have a hard time finishing their studies (more than five times higher drop-out rate) and finding employment (about half the employment rate of the national average).
There was a strong association between several objective measures of QoL (employment, living situation, and friendship) and whether or not the individual still “retained” a diagnosis of ASD, but there was no corresponding association with psychiatric comorbidity. Most parts of objective QoL (employment, living situation, romantic relationships, and friendship) were negatively associated with ASD symptom severity, except for academic success, that instead was positively associated with intelligence.
Regarding subjective feelings of QoL, a large majority (72%) had SoC scores in the average to high range, while over a quarter reported low SoC, and the mean score regarding physical HRQoL, as measured on the SF-36v2 PCS, was above average compared to norm data, and the mean score regarding mental HRQoL, as measured on the SF-36v2 MCS, was below average compared to norm data, indicating no general difficulties with physical health but clear and general difficulties with mental health. Because of the lack of studies on adults with ASDs with regard to SoC and SF-36v2, it is difficult to compare our results with empirical evidence. Compared to other measures of HRQoL (Kamp-Becker et al., 2010; Van Heijst and Geurts, 2015), the results in this study show that this cohort reports higher functioning regarding physical health but relatively similar with regard to mental health.
Regarding subjective feelings of QoL, the ASD plus group (i.e. a stable ASD diagnosis over two decades and having at least one other psychiatric disorder) scored significantly lower regarding SoC and some aspects of HRQoL, as measured on the SF-36v2. Diagnostic stability did not show an association with subjective aspects of QoL. The regression models showed that there was an association between SoC and psychiatric comorbidity (as would be suspected from the between-group analyses), but not regarding objective measures of QoL, ASD diagnostic stability, age, or intelligence.
The No longer ASD group (i.e. diagnosed with AS in childhood but not meeting criteria for a diagnosis in adult life) had objectively a higher QoL than the ASD only group (i.e. better jobs, independent living, and more friends) but did not differ from the ASD only group regarding subjective measures of QoL. The ASD plus group on the other hand did not differ from the ASD only group regarding objective measures of QoL but scored significantly worse on subjective measures of QoL. One interpretation of these results is that amount of ASD symptoms predicts how well you function in everyday life and your degree of independence, but how you feel about your life is predicted by psychiatric comorbidity. This adds to the importance of examining both objective and subjective measures of QoL when following an ASD group over time, as well as looking at both diagnostic stability and psychiatric comorbidity when examining QoL in an ASD sample.
The results of this study differ somewhat from previous studies of QoL in ASDs, we found better objective and subjective QoL than previous authors (e.g. Balfe and Tantam, 2010; Eaves and Ho, 2008; Howlin et al., 2013; Van Heijst and Geurts, 2015). The fact that our study not only includes individuals with a current ASD but also individuals with an “optimal outcome” are part of the reason for these differing results. Another aspect is the fact that this study uses a longitudinal design, whereas some other studies have used a cross-sectional study on clinical populations, meaning that they have a slightly skewed population, as most of the participants in such groups would probably fit within the definition of ASD plus (who had relatively poorer QoL in our study). Another difference between this study and other similar studies is the fact that our sample all had a clinical diagnosis of AS in childhood, whereas some studies had shown that a diagnosis of AS can be associated with better functioning than a diagnosis of autistic disorder.
Romantic relationships seemed to be the area where the No longer ASD group still showed difficulties similar to others with a stable ASD. It is plausible to assume that even though these men have clearly improved in many aspects of social and general functioning, the area of romantic relationships demand more subtle understanding of social norms that still might be difficult for some individuals with a previous ASD.
The two groups with a stable ASD diagnosis over two decades in this study studied at university at the national average, whereas the No longer ASD group studied at university at a lower level. This is somewhat surprising as the No longer ASD group would be expected to function more similar to the general population. This might in some part be related to intelligence as there was a positive correlation between intelligence and academic success. On the other hand, the mean FSIQ of the group was over 110 (i.e. high average intelligence), and because of this, one would expect the group to have studied at university at least at the same rates as the national mean.
There are some clinical implications from of this study. It is of importance for clinicians to note that the long-term prognosis of AS was extremely varied, ranging from no longer meeting criteria of ASD while functioning quite well with regard to QoL to individuals with clear ASD symptoms and low independence and QoL. Even though there was great variability, it is important to note that the vast majority of the group had a stable ASD and at least some difficulties pertaining to QoL. It is also of importance to note that subjective QoL was not related to objective QoL, but instead were related to psychiatric comorbidity. This might indicate that one way of raising the subjective QoL of men with normal range intelligence ASD is to treat their comorbid psychiatric conditions.
This study has given some ideas for future research. One area that would be of importance to study further is academic success in groups of adults with normal range intelligence ASD. In this study, 38% of the men had studied at university but 63% had dropped out without a degree (compared to 12% among average Swedish males). It would be of importance to get further insights as to why this group, despite good intellectual resources, was not able to finish their academic studies. Another important area for future research would be to investigate whether one could raise the subjective QoL of individuals with ASD and comorbidity by treating their comorbid disorder, without changing their objective QoL.
There are several strengths and limitations to this study. The main strength of the study is the overall design, that is, a representative group of males with AS followed over a period of 19 years. This has given a fairly unique opportunity to understand the natural long-term development of AS, and several different aspects of functioning have been analyzed. Another strength of this study is that both objective and subjective QoL was analyzed, giving a fairly broad understanding of the concept of QoL in adult males diagnosed with AS in childhood. The primary limitation is the high attrition rate (only 50 out of the 100 in the original cohort participated in this study). The group that chose not to participate in this study only differed as regards of intelligence (having a lower Full-Scale and Performance IQ), indicating that perhaps the sample in this study functions somewhat better than the entire group as a whole. On the other hand, intelligence showed no association with either subjective or objective QoL, meaning that perhaps the difference in intelligence is of minor importance for the results of this study. Another limitation of this study is the fact that there are only males in the study, meaning that any conclusions can only be made regarding males with AS. Also, even though this is a longitudinal study, all analysis has been made on data collected at T2, meaning that we cannot compare our results to the previous follow-up or make claims of causation, only association. Another limitation is the fact that two participants only participated by phone, and that some participants did not answer all questionnaires. Finally, it is a limitation that the statistical power calculations at the start of the study indicated the need for 100 participants and only 50 men participated in this study. This in turn means that the statistical power of the study was somewhat weak and gives some doubt regarding the statistical analyses made in this study.
To conclude, this study has shown that in a clinical cohort of males diagnosed with AS in childhood and followed up over a period of over 19 years, there was great variability in relation to both objective and subjective QoL. The subgroup that no longer met criteria of an ASD (22%) functioned quite well in regard to both subjective and objective QoL. The subgroup (48%) that still met criteria of ASD as well as at least one other comorbid diagnoses had extremely varied objective QoL (often with low independence) and low subjective QoL. Finally, the subgroup of individuals (30%) who still met criteria of ASD but not for any other psychiatric disorder also had extremely varied objective QoL (often with low independence), but the subjective QoL in this subgroup was within the average range. In the total study group, most objective QoL factors were related to ASD symptom load, except academic success which was related to intelligence.
Footnotes
Funding
The study was supported by funding from the Centre for Research and Development in Region Gavleborg and the Child and Adolescent Psychiatric Clinic in Gavle, VG Region Scientific Fund, AnnMarie and Per Ahlqvist Foundation, the Jerring Fund, Wilhelm and Martina Lundgren Foundation, Petter Silfverskiold Foundation, Golje Foundation, the Swedish Child Neuropsychiatry Science Foundation, and the Gillberg Neuropsychiatry Centre.