
Abstract
In adults with autism spectrum disorder, co-occurring psychiatric conditions are prevalent, and depression is one of the most common co-occurring disorders. This study examined the relationship between depression and cognitive ability, autism symptom severity, and self-reported social impairments in autism spectrum disorder. A total of 33 adults with autism spectrum disorder and 28 adults with typical development completed a standardized psychiatric interview, cognitive test, measure of clinician-rated autism symptom severity, and self-report of social impairments. Nine participants with autism spectrum disorder (27%) met the criteria for a depressive disorder (autism spectrum disorder + depressive disorder). Relatively more females with autism spectrum disorder had a co-occurring depressive disorder. The typical development group had a higher intelligence quotient than the autism spectrum disorder group, but the autism spectrum disorder + depressive disorder group did not differ from the typical development or autism spectrum disorder group. While the autism spectrum disorder + depressive disorder group had lower clinician-rated autism symptom severity than the autism spectrum disorder group, the autism spectrum disorder + depressive disorder group reported more social impairments than the autism spectrum disorder group. Self-reported social impairments predicted depression in adults with autism spectrum disorder when accounting for symptom severity and cognitive ability. These findings suggest that more self-perceived social impairments are related to depressive disorders in autism spectrum disorder, and may help clinicians identify individuals who are vulnerable in developing a co-occurring depressive disorder. Future directions include follow-up studies with larger cohorts and longitudinal designs to support inferences regarding directionality of these relationships.
Autism spectrum disorder (ASD) is defined by impairments in social communication and the presence of restricted and repetitive behaviors (RRBs) and atypical response to sensory information (American Psychiatric Association, 2013). In addition to these core symptoms, co-occurring psychiatric conditions are common in ASD throughout adolescence and adulthood (Buck et al., 2014; Croen et al., 2015; Ghaziuddin & Zafar, 2008; Lever & Geurts, 2016; Lugnegård, Hallerbäck, & Gillberg, 2011; Moseley, Tonge, Brereton, & Einfeld, 2011). Depression is one of the most commonly observed co-occurring conditions in adults with ASD (Ghaziuddin, Ghaziuddin, & Greden, 2002; Lever & Geurts, 2016; Lugnegård et al., 2011; Roy, Prox-Vagedes, Ohlmeier, & Dillo, 2015). The lifetime prevalence of depression in ASD is estimated to be 14%, and the current prevalence is higher than adults with typical development (TD; Hudson, Hall, & Harkness, 2018) as well as those with other psychiatric conditions (Joshi et al., 2013). A recent study following individuals up to the age of 27 years found approximately 20% of individuals with ASD had a diagnosis of depression compared to 6% of the general population (Rai, Heuvelman, et al., 2018). In the general population, depression is noted to exert a greater health burden among women (Kuehner, 2003, 2017), but sex differences in ASD are unclear, with some studies suggesting increased depressive symptoms in females (Gotham, Brunwasser, & Lord, 2015) and others indicating similarities among males and females (De-la-Iglesia & Olivar, 2015; Hudson et al., 2018).
Depression exerts a significant impact on daily functioning. In the general population, depressive disorders affect 322 million people (World Health Organization, 2017), and are a leading cause of health burdens (Ferrari et al., 2013). Depressive disorders are the largest global contributors of Years Lived with Disability (YLD), a measure of functional impairment due to a disease (World Health Organization, 2017). Depressive symptoms are often accompanied by impairments in psychosocial functioning, affecting one’s occupation and relationships (Godard, Baruch, Grondin, & Lafleur, 2012). Even when depressive symptoms remit, impairments in psychosocial functioning may remain (Kennedy, Foy, Sherazi, McDonough, & McKeon, 2007; Marangell et al., 2009). In ASD, co-occurring psychiatric conditions are also related to poorer psychosocial outcomes in both children (Chiang & Gau, 2016) and adults (Gillberg, Helles, Billstedt, & Gillberg, 2016; Hofvander et al., 2009). A specific relationship is observed between depression and poorer adaptive functioning in ASD (Kraper, Kenworthy, Popal, Martin, & Wallace, 2017; Stewart, Barnard, Pearson, Hasan, & O’Brien, 2006). Co-occurring psychopathology contributes to a larger discrepancy between adaptive functioning and intelligence quotient (IQ) for young adults with ASD (Kraper et al., 2017). A better understanding of the etiology, course, and treatment of co-occurring disorders in ASD offers a promising avenue to improve psychosocial outcomes, adaptive functioning, and quality of life for adults with ASD.
In addition to poorer adaptive functioning and psychosocial outcomes, depression is associated with increased mortality. In the general population, suicide was the leading cause of death globally among 15–29-year-olds in 2015 and accounted for close to 1.5% of deaths worldwide (World Health Organization, 2017). Individuals with ASD and co-occurring depression are at higher risk for suicidal ideation and behavior (Hedley & Uljarević, 2018) with depression representing the most common risk factor for suicidal attempts (Zahid & Upthegrove, 2017). Understanding predisposing factors and the presentation of depressive disorders in ASD holds promise to identify vulnerable individuals and to connect them to treatment, offering potentially life-saving intervention (Hedley & Uljarević, 2018).
The proposed risk factors for co-occurring depressive disorders in ASD include biological, psychological, and social factors, such as family history, gender, age, genetic factors, social relationships, and life events (for a full review, see De-la-Iglesia & Olivar, 2015; Ghaziuddin et al., 2002). Another proposed risk factor is awareness of social impairments (De-la-Iglesia & Olivar, 2015; Wing, 1981, 1996), which is described as being aware of one’s disability and differences from other groups of people. Depression in ASD has been examined in relation to cognitive ability and autism symptomology, since these two variables may influences one’s perception of their social impairments (Sterling, Dawson, Estes, & Greenson, 2008) and may act as proxy measures of “self-awareness.” Investigations into these relationships have yielded mixed results.
In children, a higher IQ was related to more depressive symptoms (Mayes, Calhoun, Murray, & Zahid, 2011; Mazurek & Kanne, 2010), yet another study did not show a relationship between IQ and depression (Strang et al., 2012). In terms of autism severity, one study reported that lower symptom severity was related to more depressive symptoms (Mazurek & Kanne, 2010), yet other studies revealed that a higher symptom severity was related to depression (Mayes et al., 2011; Rai, Culpin, et al., 2018), and another study demonstrated no relationship between symptom severity and depression (Strang et al., 2012). In a review examining depression in children and adults with ASD, samples that included individuals with an intellectual disability revealed a significantly higher rate of depression in individuals with ASD and without an intellectual disability (Hudson et al., 2018).
In studies on adults, similar inconsistencies have emerged; some studies indicated that a higher IQ was related to more depressive symptoms (Chandrasekhar & Sikich, 2015; Sterling et al., 2008) while other studies reported no relationship between IQ and depression (Cederlund, Hagberg, & Gillberg, 2010; Gotham, Unruh, & Lord, 2015). In reviews on adults specifically, adults with ASD and without an intellectual disability were more likely to have depression than adults with an intellectual disability (Hollocks, Lerh, Magiati, Meiser-Stedman, & Brugha, 2019; Rai, Heuvelman, et al., 2018). Regarding autism severity, one study reported that lower symptom severity was related to more depressive symptoms (Sterling et al., 2008).
These discrepancies may be due to the different ages studied, children versus adults, as well as the differences in the population studied, whether or not individuals with an intellectual disability were included. Another factor that may contribute to these discrepancies is the varying modalities of assessing autism severity, for example, clinician or parent report. In addition to cognitive ability and clinician report, the self-perception of social difficulties may be a clinically useful predictor of depression in ASD. Studies using self-report measures indicate that greater self-perceived autistic impairments in young adults (Gotham, Bishop, Brunwasser, & Lord, 2014) and lower self-perceived social competence in adolescents (Vickerstaff, Heriot, Wong, Lopes, & Dossetor, 2007) were related to higher depressive symptoms. Notably, discrepancies have been observed between clinicians and parents, but using both parent report and clinician observation is the gold standard for diagnosing ASD (Lemler, 2012). Thus, comparing self-report with clinician report may be clinically useful since emerging evidence suggests that discrepant reports may better predict outcomes and provide valuable additional information (Hurtig et al., 2009; Kanne, Abbacchi, & Constantino, 2009; Lerner, Calhoun, Mikami, & De Los Reyes, 2012; Ward, Sullivan, & Gilmore, 2018).
This study sought to address observed inconsistencies in prior research by studying depression in ASD in relation to self-perceived versus clinician-rated social impairments and in the context of cognitive ability. We utilized standardized clinician-administered interviews to assess autistic and depressive symptomatology and a self-report measure of social impairments to examine standardized clinician-rated symptomatology and self-perceived social impairments. Because most studies examining depression in ASD have focused on children and adolescents (Wigham, Barton, Parr, & Rodgers, 2017) we studied adults with ASD, a particularly relevant group given that the average age of onset for depression ranges from 25 to 32 years in the general population (Kessler et al., 2005). Based on the previous literature examining cognitive ability and clinician ratings in relation to depressive symptoms, we predicted that adults with ASD and depressive disorders would exhibit higher verbal cognitive ability and lower clinician-rated autism symptom severity. In addition, we predicted that adults with ASD and co-occurring depression would have more self-reported social impairments.
Methods
Participants
These data were collected as part of a larger study examining social functioning, eye-tracking, and electroencephalography across neurodevelopmental disorders in adults (R01 MH107426, James McPartland, PI). Clinical assessments and self-report measures reported here were collected over 2–3 days in this context. All participants were recruited from the greater New Haven area through flyers. In addition, participants with ASD were recruited through autism-related events and re-contacting individuals from the Yale Autism Program Research Registry with a focus on recruiting females with ASD to permit comparisons by sex. All the participants were evaluated by a trained clinical psychologist or by a master’s level clinician under the supervision of a trained clinical psychologist. Inclusion and exclusion criteria were more stringent than many clinical studies because participants were recruited according to the criteria for neuroscience research. All the participants were between 18 and 36 years old and had a full-scale IQ (FSIQ) of 70 or higher. Adults with TD were included if they did not meet criteria for any psychiatric conditions based on the Mini-International Neuropsychiatric Interview (MINI, described in detail below) and clinical judgment. Individuals with ASD were included if they met Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-V) clinical criteria for ASD, received a calibrated severity score (CSS) of four or higher on the Autism Diagnostic Observation Schedule (ADOS, described in detail below), and had no history of genetic or medical conditions etiologically related to ASD. Exclusionary criteria across groups included alcohol use in the preceding 24 h, recreational drug use in the preceding 48 h, chronic drug abuse, medication changes within the prior 2 weeks, any history of seizures (except for febrile infantile seizures), tic disorders or tremors, history of electroconvulsive therapy, bipolar disorder, and uncorrected visual, auditory, sensory-motor difficulties, neurological disorder, brain damage, or head injury. The final TD (n = 28) and ASD (n = 33) groups did not differ on gender (χ(1) = 1.63, p > 0.10) or age (t(59) = 0.55, p > 0.10). Although the ASD group had a mean IQ within the average range (M = 104, SD = 16), their FSIQ was lower than the TD group (M = 116, SD = 15), (t(58) = 3.08, p < 0.01). All procedures were conducted with the consent of participants and with approval of the Yale School of Medicine Human Investigation Committee.
Measures
Clinical assessments of depression, cognitive ability, and clinician-rated autism symptom severity were collected in addition to self-report of social impairments.
Wechsler Abbreviated Scale of Intelligence-II
The Wechsler Abbreviated Scale of Intelligence, Second Edition (WASI-II) is an abbreviated measure of cognitive ability for individuals aged 6–90 years. FSIQ was calculated based on administration of all four subtests (FSIQ-4). Since individuals with ASD often display discrepant verbal and performance IQ scores, the verbal and performance subtests were examined in addition to the FSIQ (Wechsler, 2011).
ADOS-2 module 4
The ADOS, 2nd edition (ADOS-2) is a semi-structured autism diagnostic observation with increasing modules for increasing verbal and development levels. For the verbally fluent adults in this sample, Module 4 was employed (Lord et al., 2012). The CSS, a calibrated measure of ASD symptom severity that can be compared across modules (Hus & Lord, 2014), was calculated, and individuals with a CSS of 4 or greater were included in the study.
Social Responsiveness Scale-2
The adult self-report measure, the Social Responsiveness Scale 2nd edition (SRS-2), was administered as a self-report of social impairments in ASD. The social communication and interaction (SCI) and RRB sections align with DSM-5 ASD criteria and, together, yield a total score (Constantino & Gruber, 2012). To examine the relationship between depression and self-reported social impairments in ASD, the SCI t-score was utilized.
MINI
The MINI is a brief, structured, diagnostic interview for Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) and International Classification of Diseases (ICD)-10 psychiatric disorders. Major depressive disorder (DEP) and dysthymic disorder are evaluated in the past 2 weeks and past 2 years, respectively (Hergueta, Baker, & Dunbar, 1998). No participants with TD met the criteria for any psychiatric disorders on the MINI. Participants with ASD were placed in the ASD and DEP group (ASD + DEP) if they met the MINI criteria for Major Depressive Episode, Current; Major Depressive Episode, Recurrent; Major Depressive Episode with Melancholic Features, Current; or Dysthymia, Current.
Statistical approach
Differences between the ASD, ASD + DEP, and TD groups were examined utilizing a chi-square test for sex, and one-way analysis of variance (ANOVA) with effect sizes, eta-squared (η2), and Bonferroni adjusted post hoc tests for significant findings for IQ, CSS, and SCI t-score. Since the test is sensitive to outliers, the one-way ANOVAs were examined with and without outliers. Outliers were identified as 1.5 times the interquartile range (IQR) above the third quartile or below the first quartile. A multivariate logistic regression was run to determine whether variables of interest, cognitive ability, clinician-rated autism severity, and self-reported social impairments, predicted depression status in adults with ASD.
Results
ASD and depression
Of 33 participants with ASD, nine (27.3%) met the criteria for at least one of the depressive disorders on the MINI (Table 1). Because of the small sample size, these findings are considered exploratory. There was a significant difference in sex between the groups (χ(2) = 6.0, p < 0.05). Follow-up chi-square tests revealed the ASD group had significantly fewer females (n = 4) than the TD (n = 12, p < 0.05) and ASD + DEP (n = 5, p < 0.05) groups (Table 1). A total of 5 out of 9 females with ASD (56%), compared to 4 out of 24 (17%) males with ASD, had co-occurring depression. Groups did not differ on age (F(2, 58) = 0.26, p > 0.10, η2 = 0.01), and age was not correlated with behavioral measures (Table 2).
Sex and age in the ASD, ASD + DEP, and TD groups.
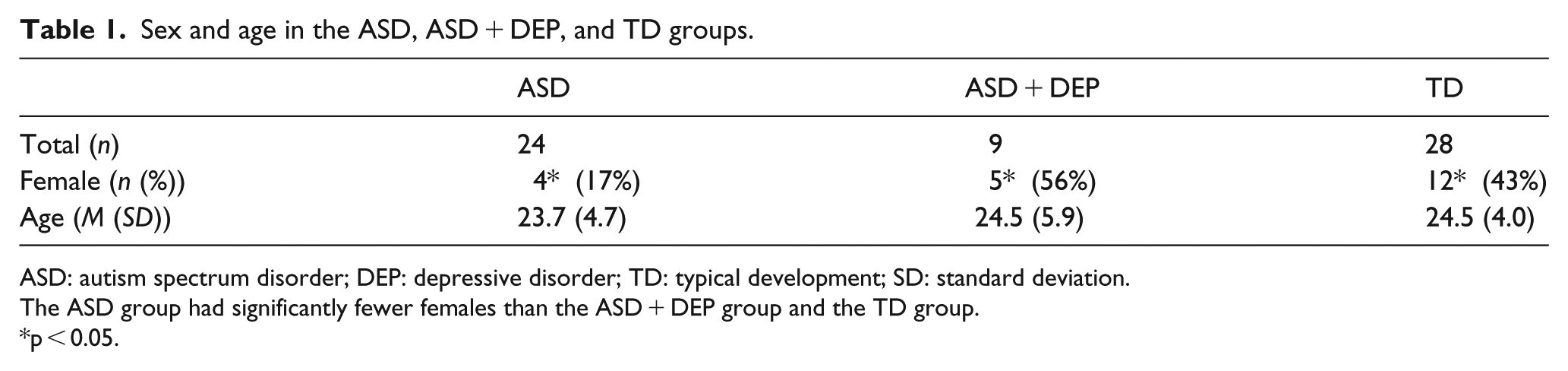
ASD: autism spectrum disorder; DEP: depressive disorder; TD: typical development; SD: standard deviation.
The ASD group had significantly fewer females than the ASD + DEP group and the TD group.
p < 0.05.
Spearman’s rank correlations across the ASD and ASD + DEP groups.
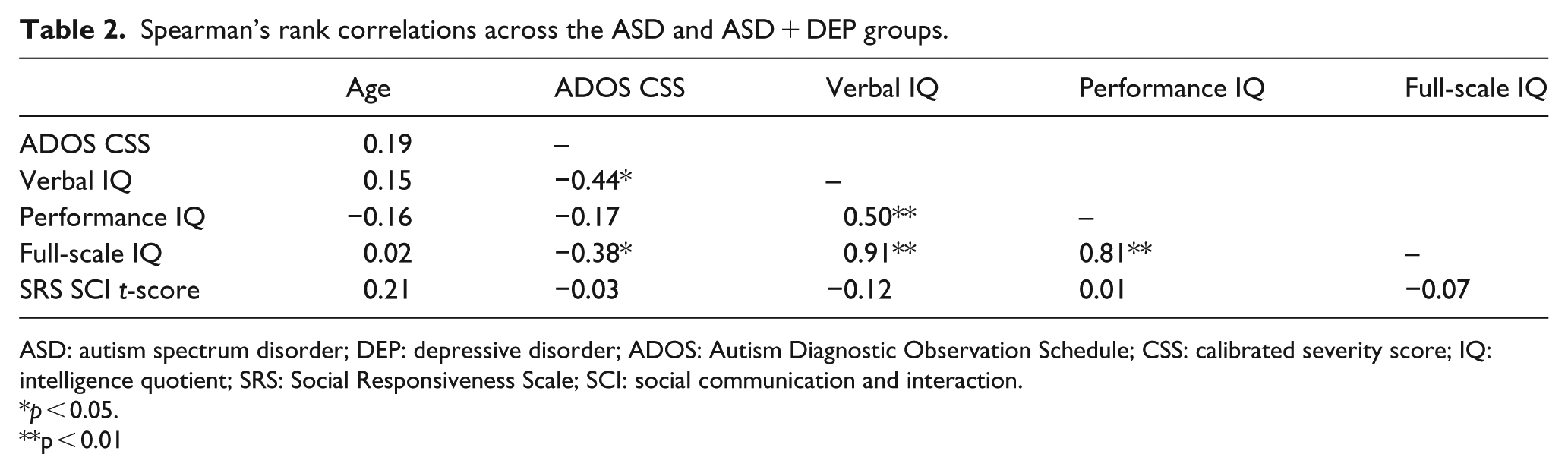
ASD: autism spectrum disorder; DEP: depressive disorder; ADOS: Autism Diagnostic Observation Schedule; CSS: calibrated severity score; IQ: intelligence quotient; SRS: Social Responsiveness Scale; SCI: social communication and interaction.
p < 0.05.
p < 0.01
Differences in cognitive ability, clinician-rated autism severity, and self-reported social impairments between the TD, ASD, and ASD + DEP groups
One-way ANOVAs with diagnosis (ASD, ASD + DEP, TD) as a between-subjects factor were carried out to determine whether differences between IQ, clinician-rated autism severity, or self-reported social impairments were present (Table 3, Figure 1). Differences in all domains emerged (ps < 0.05).
Mean scores and post hoc results in the ASD, ASD + DEP, and TD groups.
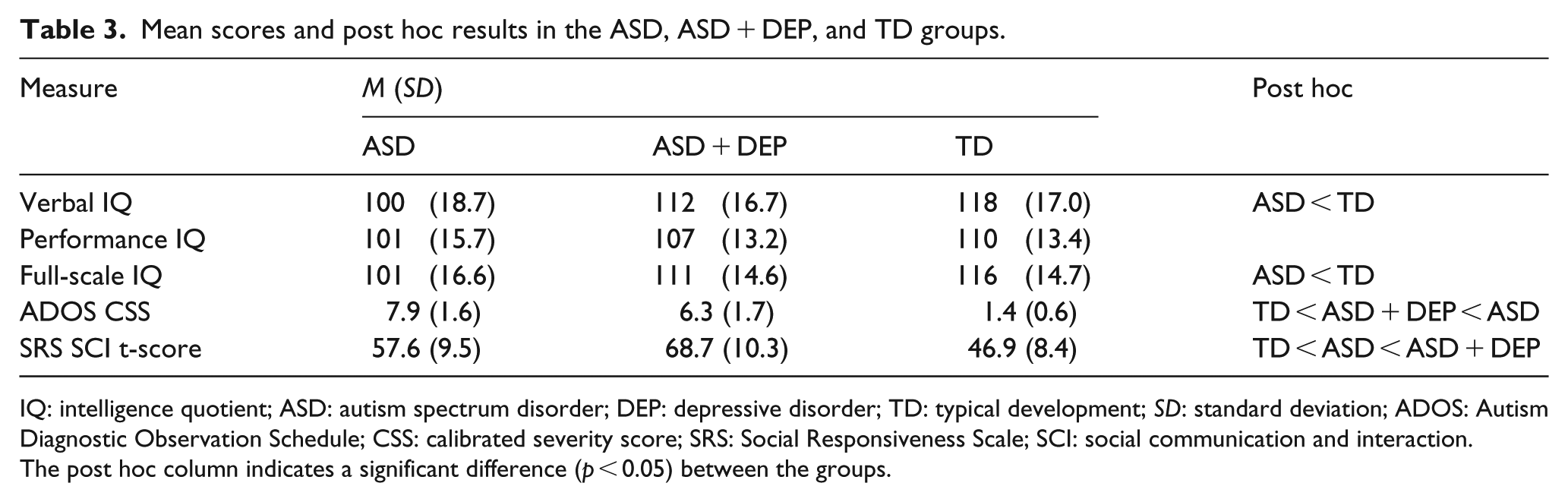
IQ: intelligence quotient; ASD: autism spectrum disorder; DEP: depressive disorder; TD: typical development; SD: standard deviation; ADOS: Autism Diagnostic Observation Schedule; CSS: calibrated severity score; SRS: Social Responsiveness Scale; SCI: social communication and interaction.
The post hoc column indicates a significant difference (p < 0.05) between the groups.

Boxplots of (a) full-scale IQ, (b) ADOS CSS, and (c) SRS SCI t-score by group.
Cognitive ability
Differences in verbal (F(2, 57) = 6.92, p < 0.01, η2 = .20) and full-scale (F(2, 57) = 6.31, p < 0.01, η2 = 0.18) IQ emerged. The ASD + DEP group did not differ from the ASD or TD group on verbal or FSIQ (Figure 1(a), ps > 0.10). The ASD group had significantly lower verbal and FSIQ than the TD group, and these findings remained significant after outliers were removed (ps < 0.05). No differences in performance IQ were observed (F(2, 57) = 2.45, p = 0.10, η2 = 0.08).
Clinician-rated autism severity
The groups differed on CSS (F(2, 58) = 177.5, p < 0.01, η2 = 0.86) such that the TD group had significantly lower scores than both the ASD and ASD + DEP groups (Figure 1(b), ps < 0.05), and the ASD + DEP had significantly lower scores than the ASD group (p < 0.05).
Self-reported social impairments
On the SRS, groups differed on the SCI t-score (F(2, 57) = 21.8, p < 0.01, η2 = 0.43). The TD group had significantly lower scores, indicating fewer self-reported social impairments compared with the ASD and ASD + DEP groups (Figure 1(c), ps < 0.05), and the ASD group had significantly lower scores than the ASD + DEP group (p < 0.05). These findings remained significant after outliers were removed (ps < 0.05).
Relationships among cognitive ability, clinician-rated autism severity, self-reported social impairments, and depression in ASD
Relationships among cognitive ability (FSIQ), clinician-rated autism severity (CSS), self-reported social impairments (SCI t-score), and depression were examined with multivariate logistic regression. A multivariate logistic regression was performed with the diagnosis of depression as the outcome variable, and cognitive ability, clinician-rated autism severity, and self-reported social impairments in adults with ASD (Table 4) as the predictors The model indicated that self-reported social impairments were associated with depression in adults with ASD (Figure 2, p < 0.05) with an odds ratio of 1.16 (95% confidence interval (CI) = 1.04–1.39), such that, for an increase of 1 point on the SCI t-score, the odds of having depression increased by a factor of 1.16. Clinician-rated autism severity was marginally associated with depression in adults with ASD (p = 0.08) with an odds ratio of 0.55 (95% CI = 0.26–1.01). However, there was no association with cognitive ability (p = 0.18) and the odds of having depression, 1.05 (95% CI = 0.98–1.14).
Predictors of depression in adults with ASD: results from multivariate regression model.

OR: odds ratio; CI: confidence interval; IQ: intelligence quotient; ADOS: Autism Diagnostic Observation Schedule; CSS: calibrated severity score; SRS: Social Responsiveness Scale; SCI: social communication and interaction; VIF: variance inflation factor.
p < 0.10.
p < 0.05.

Multivariate logistic regression in adults with ASD with depression diagnosis as the outcome variable where 0.00 indicates low probability of receiving a depression diagnosis.
Discussion
This study examined the relationship between co-occurring depression and cognitive ability, clinician-rated autism severity, and self-perceived social impairments in adults with ASD. A structured diagnostic interview was utilized to determine the presence of co-occurring depressive disorders in individuals with ASD. Contrary to our hypotheses, adults with ASD and depressive disorders did not differ from either adults with ASD or adults with TD on measures of cognitive ability. However, as predicted, adults with ASD and depressive disorders exhibited lower clinician-rated autism severity yet more self-reported social impairments than adults with ASD.
The rate of depressive disorders in this sample of adults with ASD (27.3%) was consistent with a recent meta-analysis of depression in studies that used a standardized, self-reported assessment of current depressive symptoms (25.9%, 95% CI = 17.0–37.3; Hudson et al., 2018). While other studies have not found sex differences (De-la-Iglesia & Olivar, 2015; Hudson et al., 2018), here, we observed a greater proportion of females among individuals with depression and ASD (compared with ASD alone). Emerging evidence suggests females with ASD show a greater increase in depressive and anxiety symptoms throughout adolescence (Gotham, Brunwasser, & Lord, 2015), and a study in adults with ASD utilizing a self-report of depression found that significantly more women than men had depression (Gotham, Unruh & Lord, 2015). This highlights the importance of examining sex differences after puberty since the relationship between changes in estrogen and androgen to depressive symptoms in ASD are potentially relevant but poorly understood (Ghaziuddin et al., 2002). Furthermore, in the general population (Brody, Pratt, & Hughes, 2018), the prevalence of depression in females (10%) and males (6%) is considerably lower than the rates in this study for females with ASD (56%) and males with ASD (17%). Higher rates of depression in females is observed in the general population and this study, and the burden of depression in ASD across sexes demonstrates the need to identify effective diagnostic measures and treatments for depression in ASD.
Cognitive ability, clinician-rated autism severity, and self-perceived social impairments in relation to depressive symptoms were also examined. Contrary to another study in adults with ASD, differences in verbal and FSIQ between the ASD group and ASD and depressive disorders group were not found (Sterling et al., 2008). Of note, while the ASD group did have a significantly lower IQ than the TD group, the ASD and depressive disorders group did not significantly differ from the TD group. If differences between the ASD and depressive disorders group and the ASD or TD groups exist, this study may have been underpowered to detect these differences. The null findings in this study may also reflect the inclusion criteria since this study required IQ greater than or equal to 70 while the Sterling and colleagues study included individuals with FSIQ as low as 57. The failure to detect a significant relationship between cognitive ability and depression is consistent with other studies with an IQ ⩾ 70 inclusion criteria (Cederlund et al., 2010; Gotham, Unruh & Lord, 2015; Strang et al., 2012).
Regarding the relationship between clinician-rated autism severity and depression, we found lower clinician-rated autism severity as measured by the ADOS-2 CSS in adults with ASD and depressive disorders compared with adults with ASD. A similar relationship between lower autism severity and depression was also found in prior samples of children and adolescents (Mazurek & Kanne, 2010) and adults (Sterling et al., 2008). Because the CSS can be scored across modules and relative to language and age level, future longitudinal studies examining the development of depression in ASD can utilize the CSS to determine the direction of the relationship between autism symptom severity and depression.
Finally, our results indicated that greater self-reported social impairments were predictive of depression. Notably, the mean SRS SCI t-score for the ASD group was in the normal range, while the mean score of the ASD and depressive disorders group was in the moderate range, that is, symptoms are “clinically significant and lead to substantial interference with everyday social interactions” (Constantino & Gruber, 2012). Interference with social interactions has been studied in children, indicating children with low self-perceived social competence have more depressive symptoms (Vickerstaff et al., 2007). This may signify that depressive symptoms lower the view of one’s social abilities as indiciated by more self-reported social difficulties. Yet the current results demonstrate a contradictory pattern between self-reported versus clinician-rated autism severity. We interpret the relationship among greater self-reported symptomatology and depression (despite lower clinician-rated severity) as evidence for the potential influence of self-perception on development of depressive symptomatology. In other words, individuals who, even potentially inaccurately, see themselves as more severely impacted, may be at greater risk for depression.
The finding that lower clinician-rated autism severity was associated with depression may, in part, reflect the specific items contributing to the clinician score. For example, “insight” is an item on the ADOS-2, with a lower score indicating more typical understanding of social relationships. An individual with a better understanding of typical relationships and social communication may be more likely to perceive their behavior as atypical. Clinicians working with individuals who report more social impairments should be vigilant for depressive problems even if clinician perception of autistic symptoms indicates reduced severity. The cross-sectional nature of this study precludes verification of this interpretation, so we consider this interpretation hypothesis-generating and requiring confirmation in studies designed to support directional influence.
We identified a number of factors related to co-occurring depression in ASD including female sex, lower clinician-rated autism severity, and more self-reported social impairments in adulthood. Using widely administered measures, the ADOS-2 and SRS-2, these findings are readily translatable for future studies in larger cohorts and longitudinal samples. Furthermore, the pattern of lower severity as per clinician report and higher self-perceived difficulties may represent a potential clinical marker indicating risk for depressive disorders. Given the link between depressive disorders and reduced adaptive function and increased suicide risk, understanding the presentation of depression in ASD may yield significant public health benefits, including improvement in psychosocial outcomes and adaptive functioning.
This study had a number of limitations. As previously mentioned, the study is cross-sectional, therefore, longitudinal studies are necessary to determine the directionality of these relationships. For example, we found a relationship between self-reported social impairments and depression in ASD, but we cannot determine whether this self-perception preceded the development of depression or vice versa. Longitudinal or sufficiently large studies can determine whether awareness of social impairments is a risk factor for later developing depression, or a marker of current depression. Another limitation is the small sample size; thus, this study may be underpowered to detect differences (i.e. higher IQ and depression). While there was an increased odds of more self-reported social impairments in adults with ASD and depression, the confidence interval approached one, highlighting the need for larger samples to confirm this result. Larger sample sizes will also allow for more complex models to test the potential moderating effects of factors such as age, sex, and cognitive ability. In future studies a depression group is critical, since it is likely more similar to the ASD + DEP group compared to the TD group, and therefore may allow for the identification of the similarities, or lack thereof, in the presentation of depression in ASD. The study excluded individuals with an IQ below 70, and required individuals to verbally express their experiences, on the MINI, and self-report, on the SRS. These requirements preclude many individuals on the spectrum, therefore other risk factors for co-occurring depression should be explored for these groups.
This study suggests that more self-reported social impairments and lower clinician-rated autism severity are related to depression in adults with ASD. The relationship between cognitive ability and depression is still unclear, since adults with ASD and depression did not differ from either adults with ASD or adults with TD. Clinicians can utilize these features, more self-reported social impairments and lower clinician-rated autism severity, to identify individuals with ASD at risk for developing depressive disorders.
Supplemental Material
AUT857375_Lay_Abstract – Supplemental material for Self-reported social impairments predict depressive disorder in adults with autism spectrum disorder
Supplemental material, AUT857375_Lay_Abstract for Self-reported social impairments predict depressive disorder in adults with autism spectrum disorder by Talena C Day, Kathryn A McNaughton, Adam J Naples and James C McPartland in Autism
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the NIMH, Project No.: 5R01MH107426.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.