
Abstract
More adults are undergoing autism assessment due to recent changes in awareness, diagnostic criteria and professional practices. This scoping review aimed to summarise research on autism diagnosis in adulthood and identify any gaps for future study. The authors searched for studies involving first-time assessment and diagnosis of autism in adults, which identified 82 studies from 13 countries using various methodologies. Six themes of (1) prevalence, (2) diagnostic pathways and processes, (3) gender, (4) psychosocial characteristics, (5) co-occurring conditions and (6) experiences of diagnosis were identified across the studies. Findings suggest that receiving an autism diagnosis has a significant emotional impact on adults, but accessibility and processes are inconsistent, and formal support services are lacking. More research is needed on autism diagnosis in adults with intellectual disability, consequences of the timing of diagnosis, and support after diagnosis.
Lay abstract
More adults are getting assessed for possible autism. Here, we give an overview on what is already known about autism diagnosis in adulthood and find areas that need more research. We divided results from the studies we found into six topics of (1) rates of autism in different groups; (2) the process of getting an autism diagnosis in adulthood; (3) gender; (4) personality traits, abilities and behaviours of diagnosed adults; (5) mental and physical health conditions that occur together with autism; and (6) how adults think and feel about being assessed and diagnosed. We found that adults often have strong emotions after being diagnosed, the process of getting a diagnosis can be unclear and different for everyone, and not many support services are available for adults. More research on diagnosing adults with intellectual disability, differences between early and late-diagnosed adults, and support after diagnosis would be useful.
Autism’s conceptual expansion, broadening of diagnostic criteria and increased awareness have resulted in a ‘lost generation’ whose autism remained undetected until adulthood (Lai & Baron-Cohen, 2015, p. 1013). Adult autism assessment involves unique challenges. As diagnosis relies on knowledge of developmental history, adults and families’ lack of access to early medical records and inaccurate recall of developmental milestones are significant difficulties (Lai & Baron-Cohen, 2015; Rutherford, McKenzie, Forsyth, et al., 2016). Furthermore, autistic adults sometimes use learned coping strategies that reduce the impact of autistic traits on everyday functioning, known as ‘camouflaging’ (Lai et al., 2017, p. 690). Adults seeking diagnosis may undergo multiple consultations with different health professionals (Jones et al., 2014) and experience lengthy waiting times (Rutherford, McKenzie, Johnson, et al., 2016). Although autism diagnosis has become more widely available, adults still encounter barriers to efficient diagnosis and appropriate support.
The National Institute for Health and Care Excellence (NICE) in the United Kingdom and the Cooperative Research Centre for Living with Autism (Autism CRC) in Australia have both published guidelines on assessment, diagnosis and support of adults on the autism spectrum (NICE, 2012; Whitehouse et al., 2018). Both include information on how autistic traits present in adults and recommend multidisciplinary assessment by trained professionals, with some differences in recommended assessment processes. A recent systematic review of autism assessment guidance documents further notes publications from governments and organisations in the United States, Canada and New Zealand (Penner et al., 2018), though it did not discuss recommendations for adults.
Existing reviews on adult autism diagnosis tend to focus on evaluating screening measures and diagnostic tools (Baghdadli et al., 2017; Falkmer et al., 2013; Hirota et al., 2018). Several systematic reviews examined characteristics of autistic adults, but did not address adulthood diagnosis (Jacob et al., 2015; Kirby et al., 2016; Magiati et al., 2014). Systematic reviews involving both children and adults lacked discussion specific to each age group (Daniels & Mandell, 2014; I. Smith et al., 2015). One systematic review from the United Kingdom discussed autism diagnosis in adults (Hayes et al., 2018), but focused exclusively on clinical guidance documents. A review that comprehensively synthesises evidence from a variety of sources on autism diagnosis in adulthood is needed.
Research into adult autism diagnosis varies greatly in topics and methodologies. This heterogeneity lends itself to a scoping review approach to integrate the diversity of research in this emerging area (Arksey & O’Malley, 2005). Unlike a traditional systematic review addressing a specific research question, a scoping review summarises research in a broader area in a rigorous and transparent manner (Arksey & O’Malley, 2005; McKinstry et al., 2014). This scoping review aimed to provide an overview of research on adult autism diagnosis, discuss themes and identify gaps for future study.
Method
This scoping review was constructed from the research question ‘What is known from existing research on the diagnostic pathways, processes, characteristics and experiences of people diagnosed with autism in adulthood?’ based on Arksey and O’Malley’s (2005) framework for scoping studies, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) (Tricco et al., 2018) and the Joanna Briggs Institute (JBI) Reviewer’s Manual (Peters et al., 2017). The protocol was registered on Open Science Framework under the DOI 10.17605/OSF.IO/DB78Q.
Eligibility criteria
Scoping reviews may include grey literature and non-academic sources (Arksey & O’Malley, 2005). However, the authors decided to only include published primary studies. Due to the large quantity of existing studies and systematic reviews on screening and diagnostic measures (e.g. Baghdadli et al., 2017; Falkmer et al., 2013), the authors excluded studies that exclusively report on the psychometric properties of these tools.
The following inclusion criteria were used:
Topic involves diagnosis of autism spectrum disorder (ASD) or Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV)/International Statistical Classification of Diseases and Related Health Problems (10th ed.; ICD-10) subtypes.
Population involves people who underwent or are seeking a first-time autism diagnosis in adulthood, their carers or professionals who diagnose adults. (a) For studies where the population includes autistic adults, there is a sample or subsample where mean age of diagnosis ⩾18 years.
Contains findings specific to diagnosis of autism occurring in adulthood. (a) In studies involving other populations or topics, findings specific to the eligible population or topic must be presented separately for at least one analysis to allow for extraction.
In qualitative studies, findings specific to the eligible population or topic must be presented separately.
Published primary studies with sample size > 1.
English language.
Published between 2008 and 2018.
Articles were excluded if they
Exclusively report on the validity, reliability, sensitivity or specificity of biomarkers, screening measures or diagnostic tools.
Search strategy
A search strategy was devised and performed in the databases Medline, Embase, PsycINFO and CINAHL. The search strategy used ‘OR’ to combine outputs from two strategies using subject headings (MeSH), and keywords with proximity operators, respectively. This search strategy was applied to all four databases, substituting for equivalent terms where the same term was unavailable (see Appendices A and B in Supplementary Material). Only the keywords with proximity operators search were performed for PsycINFO as “Diagnosis” was not available as a subheading.
As autism diagnosis in adulthood is a relatively recent phenomenon, search output was limited to English-language papers published in the past 10 years (2008–2018). Alerts for new articles were created for each database. The final search was performed on 28 November 2018.
The reference and citation lists of included studies were used to locate additional eligible studies.
Study selection
After removing duplicates, the first author screened titles and abstracts to remove ineligible records. The full texts of remaining records were then screened independently by the first and second authors. The two authors had an agreement rate of 85% and discussed any disagreements to reach a consensus. Disagreements mainly involved articles with ambiguity over whether participants had previous autism diagnoses. These articles were included if they also included participants receiving an initial diagnosis.
The citation and reference lists of included articles were screened by the first author.
Data extraction
The authors developed a data extraction chart based on Arksey and O’Malley’s (2005) charting form and the Cochrane Collaboration’s guidance on extracting qualitative evidence (Noyes & Lewin, 2011) to account for a variety of research designs. The first author charted all included papers.
The following data items were extracted from studies: (1) participant characteristics; (2) setting and context; (3) phenomena of interest and aims; (4) study design, method and data analysis; (5) results and original authors’ interpretations; and (6) limitations.
Critical appraisal
The first author appraised all included studies for quality. Quantitative studies were appraised using the JBI Critical Appraisal Tools (JBI, 2017). The JBI provides checklists for several types of quantitative and qualitative health research design examining aspects of quality such as sampling, measures and data analysis. The Qualitative Checklist from the Critical Appraisal Skills Programme (CASP) set of tools for evaluating healthcare research (CASP, 2018) was chosen instead of the JBI Checklist for Qualitative Research due to greater relevance of items on research design and methodology. Mixed-methods studies were appraised using the Mixed Methods Appraisal Tool (Hong et al., 2018), which assesses the integration of quantitative and qualitative components. As the scoping review aims to present an overview of existing research regardless of the quality of individual studies (Arksey & O’Malley, 2005), no study was excluded due to quality.
As the checklists for each study design contain varying numbers of items, a mean score of all items in the relevant checklist is calculated for each included study. Each ‘yes’ was assigned a score of 2, ‘no’ a score of 0, and ‘unclear/can’t tell’ a score of 1. Although there are no standardised cut-off scores for quality appraisal checklists, the authors consider a mean score of ⩾1.5 to indicate high quality, based on the distribution of scores in included studies.
Synthesis of results
Findings from studies were organised into areas of interest based on charted phenomena of interest according to Arksey and O’Malley’s (2005) method. The first author then identified tentative overarching thematic categories across studies, which were further refined following input from the second and third authors. A numerical analysis of the characteristics of included studies was performed. The findings related to each theme were then synthesised.
Results
Study selection
Figure 1 shows a flowchart of the study selection process. The final list contains 82 studies.
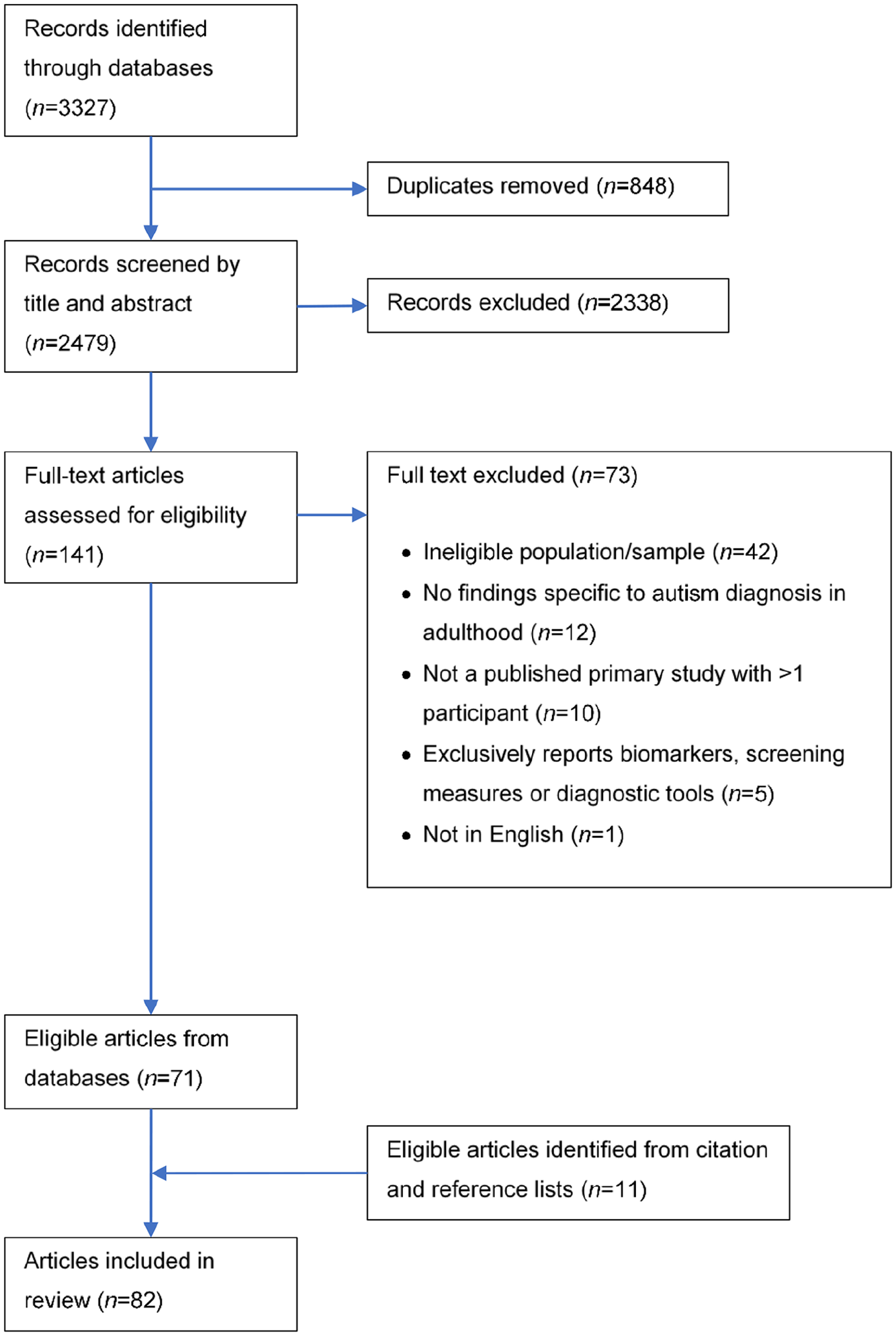
Study selection process.
Study characteristics
The 82 studies consisted of 62 quantitative, 16 qualitative, and 4 mixed-methods studies. The majority were based in the United Kingdom (39%), followed by the United States (12%) and Sweden (10%). The number of studies meeting inclusion criteria showed an increasing trend in recent years, surging in 2016 and 2018 (Figure 2).
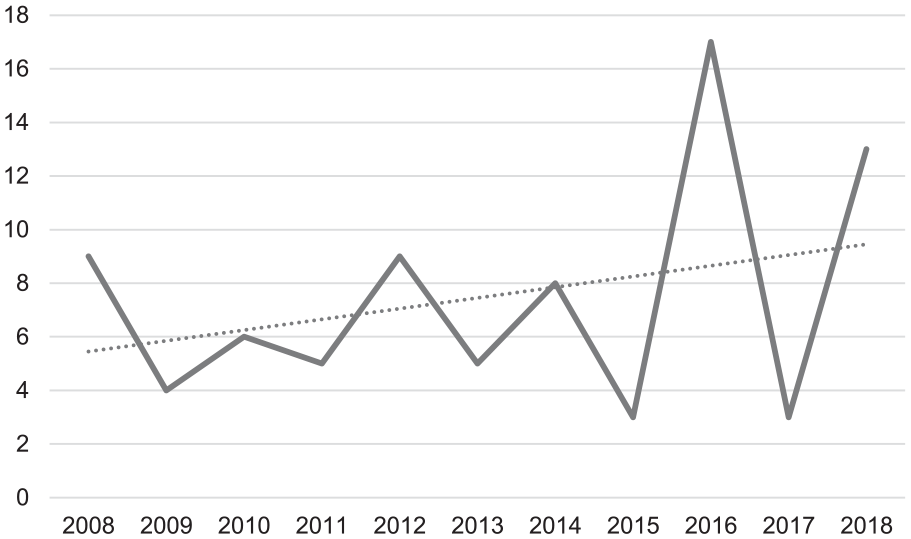
Number of included studies by year of publication.
The first author initially identified 15 areas of interest from charted data on phenomena of interest, which were combined into six themes of (1) prevalence, (2) diagnostic pathways and processes, (3) gender, (4) psychosocial characteristics, (5) co-occurring conditions and (6) experiences of diagnosis (Figure 3).
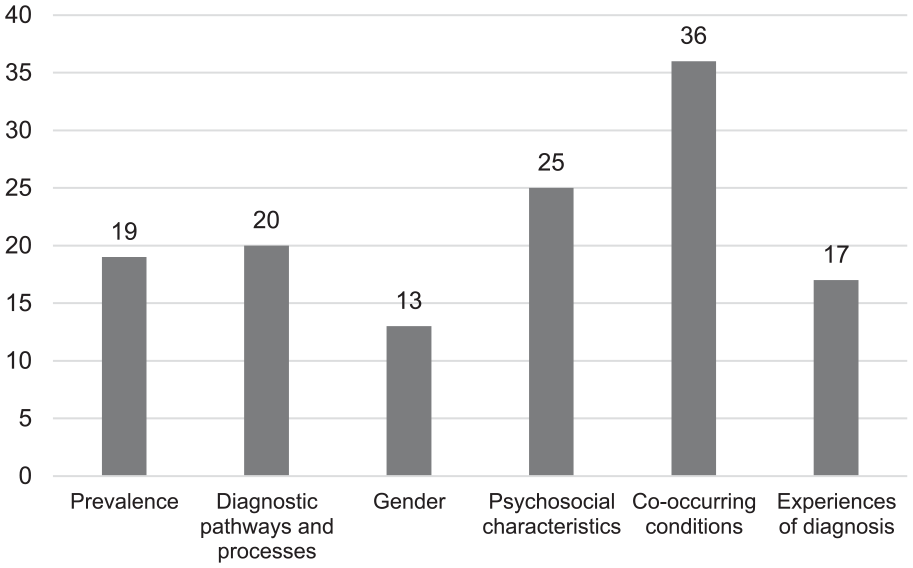
Frequency of studies related to each theme.
Details of the 82 included studies are shown in Appendix C in Supplementary Materials.
Quality appraisal
The included studies had a mean quality appraisal score of 1.54 (range = 0.89–2.00). 61% of studies attained a score ⩾1.5, indicating that the overall quality is high.
Prevalence
Nineteen studies of moderate-to-high quality (range = 1.2–2.0) estimated autism prevalence in several adult populations. The majority of studies were conducted in Europe (n = 15), including six from the United Kingdom. Several studies only included young adult age groups (Davidson et al., 2014; Diallo et al., 2018; Pinto-Martin et al., 2011; Unenge Hallerback et al., 2012), and one study used a mixed adolescent–adult sample (Kocovska et al., 2012). Most studies (14/19) performed diagnostic assessment in a sample to estimate prevalence (e.g. Brugha et al., 2011), while five studies used medical records and/or population health data to establish prevalence (e.g. Bachmann et al., 2018). Studies were inconsistent and sometimes unclear in reporting demographics and co-occurring conditions of the whole sample and the identified autistic subsample, making comparison of participant characteristics across studies difficult. Most studies involved male-majority (n = 9, >60% male) or equal-gender (n = 5) whole samples (n = 4 not stated), with one study using a male-only sample (McCarthy et al., 2015). The identified autistic subsample tended to be male-majority (n = 16, n = 2 not stated). Nine studies specified inclusion of participants with intellectual disability. Eleven studies reported co-occurring conditions other than intellectual disability in the autistic subsample. Studies examining autism prevalence in people with specific conditions were synthesised separately in the ‘co-occurring conditions’ theme.
A large UK epidemiological study estimated autism prevalence among adults living in the community to be 9.8 per 1000 (Brugha et al., 2011), adjusted to 11 per 1000 following inclusion of a sample with intellectual disability (Brugha et al., 2016). Data from several countries show the estimated prevalence and incidence of autism diagnoses in adults increased in recent years (Bachmann et al., 2018; Diallo et al., 2018; Jensen et al., 2014; Schendel & Thorsteinsson, 2018). Kocovska et al. (2012) identified 24 new autism cases in a 7-year follow-up of a child autism screening study. Studies involving data from multiple adolescent and adult age groups show that prevalence decreases as age increases (Bachmann et al., 2018; Jensen et al., 2014; Poovathinal et al., 2016; Schendel & Thorsteinsson, 2018).
There is conflicting evidence on whether autism prevalence in adult psychiatry services is higher than the general population due to variation in service characteristics and study design. A study of psychiatric inpatients at a US state hospital showed elevated rates (9.9%) of autism (Mandell et al., 2012), while the adult psychiatry register at a Swedish university hospital recorded a much lower prevalence of 1.3% (Nylander et al., 2013). The percentage of new adult autism diagnoses at the Swedish hospital increased sharply in 1998 and continued to increase gradually (Nylander et al., 2013).
Autism prevalence is elevated in several other populations, though studies investigating these groups tended to have smaller sample sizes and lower quality scores as a result. Studies of prisoners estimated autism prevalence to be 3%–5% (Enayati et al., 2008; McCarthy et al., 2015), with higher prevalence in male arsonists (Enayati et al., 2008). Pinto-Martin et al. (2011) reported a 5% autism prevalence in a cohort of young adults with low birth weight.
Diagnostic pathways and processes
Twenty studies examined the pathways and processes of adult autism diagnosis from service user (e.g. Jones et al., 2014) and provider (e.g. Rutherford et al., 2018) perspectives, as well as the impact of Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) criteria on diagnosis (e.g. Wilson et al., 2013). The majority (13/20) were conducted in the United Kingdom. The studies used a variety of designs and sources of information, including diagnostic service data (e.g. Geurts & Jansen, 2012; Young & Rodi, 2014), self-report surveys (e.g. Jones et al., 2014) and interviews (e.g. Griffith et al., 2012). Quality appraisal scores (range = 1.0–2.0) and methodological shortcomings also varied considerably among this diverse group of studies. Almost all studies involved autistic adults, except one study on carers (Raymond-Barker et al., 2018) and two on diagnosing professionals (Rogers et al., 2016; Rutherford, McKenzie, Forsyth, et al., 2016). Of the studies involving autistic adults, 12 used male-majority samples, 6 reported inclusion of participants with intellectual disability and 5 reported data on co-occurring conditions other than intellectual disability.
Adults’ initial concerns that prompted assessment were most likely to be challenges with social interactions and/or mental health (Geurts & Jansen, 2012; Jones et al., 2014). Qualitative studies involved adults who sought an assessment due to existing concerns (Crane et al., 2018), and those were prompted by their parents (Raymond-Barker et al., 2018) or partners (Lewis, 2017b). A US-based international survey of mostly female formally diagnosed and self-diagnosed adults revealed fear of not being believed by health professionals (reported by 94.4%) and difficulty finding an adult autism specialist (reported by 85.6%) deterred adults from professional assessment (Lewis, 2017a). Adults’ perceived barriers also differed by country. In the aforementioned survey, US adults viewed the cost of an autism assessment as a strong deterrent, while UK and Canadian adults viewed waiting times as a more significant barrier (Lewis, 2017a).
Referral via general practitioners (GPs) and mainstream mental health professionals were common pathways to adult autism diagnosis, as shown by data from self-report surveys (Jones et al., 2014) and diagnostic service records (Happé et al., 2016; Hofvander et al., 2009; Nydén et al., 2010; Wilson et al., 2016). Diagnostic service-based studies did not typically differentiate by referral pathway in their analysis of outcomes. Both quantitative and qualitative studies described adults who received prolonged mental health treatment before obtaining an autism assessment (Bargiela et al., 2016; Geurts & Jansen, 2012; Punshon et al., 2009; Raymond-Barker et al., 2018), with over 60% citing poor past experiences with mental health professionals and previous misdiagnosis as barriers in Lewis’ (2017a) survey. Adults and parents described that professionals not recognising signs of autism and multiple referrals resulted in delays before and during assessment (Bargiela et al., 2016; Griffith et al., 2012; Jones et al., 2014; Raymond-Barker et al., 2018). Due to these issues, there is often a gap of several years between first concern, professional consultation and diagnosis (Begeer et al., 2013; Jones et al., 2014).
Several studies from the United Kingdom examined adult assessment processes within autism diagnostic services. In a survey of 116 health professionals involved in autism diagnosis, Rogers et al. (2016) found around half of health professionals involved in adult diagnosis were satisfied with service accessibility. A large project examined assessment processes and factors influencing diagnosis duration in Scottish services (McKenzie et al., 2015, 2016; Rutherford et al., 2018; Rutherford, McKenzie, Forsyth, et al., 2016; Rutherford, McKenzie, Johnson, et al., 2016). Adult services were less likely to use standardised assessment tools than children’s services (Rutherford, McKenzie, McClure, et al., 2016). Adults experienced a mean duration of 159.2 days between referral and receiving a diagnosis (McKenzie et al., 2015). Diagnosis duration was unrelated to client gender (Rutherford, McKenzie, Johnson, et al., 2016) or service adherence to NICE guidelines (McKenzie et al., 2016), but client characteristics including intellectual disability and additional support needs predicted longer duration (McKenzie et al., 2015). A 12-month intervention co-developed by Rutherford et al. (2018) and 11 adult diagnostic services (Rutherford, McKenzie, Forsyth, et al., 2016) reduced total duration by a mean of 29.9 days. Efficient diagnostic processes benefit adults undergoing autism assessment as longer duration was associated with reduced satisfaction (Jones et al., 2014).
Diagnostic criteria
Four studies published between 2012 and 2014 examined the effect of DSM-5 autism criteria changes on adult diagnosis by retrospective analysis of data from adults diagnosed under previous criteria (e.g. Wilson et al., 2013). All except Young and Rodi (2014) used earlier proposed versions rather than the full DSM-5 criteria released in 2013. A methodological flaw common to these studies is that participants’ ICD-10/DSM-IV outcomes were not hidden from evaluators applying DSM-5 criteria. In adults with and without intellectual disability, between 22% and 62% of people who met Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR) criteria for an autism subtype did not meet criteria for DSM-5 ASD (Beighley et al., 2014; Matson et al., 2012; Wilson et al., 2013; Young & Rodi, 2014). Compared to adults who met DSM-IV or ICD-10 criteria only, meeting DSM-5 ASD criteria was associated with higher rates of obsessive-compulsive disorder (OCD) in adults without intellectual disability (Wilson et al., 2013), as well as greater overall autistic traits and stereotypic behaviours in adults with intellectual disability (Beighley et al., 2014; Matson et al., 2012).
Gender
Thirteen studies explored gender differences in adulthood diagnosis and discussed issues specific to women. This relatively small group of studies were generally high in quality (range = 1.4–2.0). Two qualitative studies involved female-only samples (Bargiela et al., 2016; Kanfiszer et al., 2017), while other studies analysed gender differences in mixed-gender samples. Four studies specified inclusion of participants with intellectual disability. Five studies provided data on co-occurring conditions other than intellectual disability among participants, and a further three examined self-reported depression/anxiety symptomology.
Although autism is predominantly diagnosed in male children, the proportion of females receiving diagnosis increased with age (Rutherford, McKenzie, Johnson, et al., 2016). Diagnostic services tended to report a male-to-female ratio of 2–3 to 1 (e.g. Happé et al., 2016; Rutherford, McKenzie, Johnson, et al., 2016; Wilson et al., 2016). Gender ratio (1.2:1) was close to equal in studies assessing autism in adults with intellectual disability (Brugha et al., 2016; Rutherford, McKenzie, Johnson, et al., 2016). Although adults identifying as transgender and/or non-binary genders participated in adult autism diagnosis studies (Lewis, 2017a; Tan, 2018), there is little literature on how this population may differ from cisgender autistic men and women.
The potential under-detection of autism in women has led researchers to examine characteristics of adulthood-diagnosed women and gender differences. Even though age of diagnosis and duration from referral to diagnosis were similar between men and women (Begeer et al., 2013; Geurts & Jansen, 2012; Lehnhardt et al., 2016; Rutherford, McKenzie, Johnson, et al., 2016), women reported greater distrust of health professionals and difficulty finding diagnosticians specialising in their gender (Lewis, 2017a). Women tended to self-report more autistic traits (Happé et al., 2016; Lehnhardt et al., 2016), but scored similar to men on clinician-rated diagnostic tools (E. Rydén & Bejerot, 2008; Wilson et al., 2016). There is no conclusive evidence of gender differences in IQ (Lehnhardt et al., 2016; Nydén et al., 2010; Wilson et al., 2016), executive function (Lehnhardt et al., 2016; Nydén et al., 2010), psychosocial functioning (Baldwin & Costley, 2016; E. Rydén & Bejerot, 2008) or mental illness (Geurts & Jansen, 2012; Russell et al., 2016; Wilson et al., 2016). Although autistic traits share more similarities with Cluster A and C personality disorders (PDs), two studies with moderately small numbers of female participants (n = 45 and n = 41, respectively) have reported on a possible overlap between autism and borderline PD in women (E. Rydén & Bejerot, 2008; G. Rydén et al., 2008).
Two qualitative studies (Bargiela et al., 2016; Kanfiszer et al., 2017) and one mixed-method study (Baldwin & Costley, 2016) explored the subjective experiences of adulthood-diagnosed autistic women. Women described putting great effort into social skills, relationships and ‘pretending to be normal’ (Baldwin & Costley, 2016; Bargiela et al., 2016, p. 3287), but some still reported significant social difficulties and desire for support to improve social skills (Baldwin & Costley, 2016; Kanfiszer et al., 2017). Experiences of bullying have been frequently reported by adulthood-diagnosed women (Bargiela et al., 2016; Hofvander et al., 2009; Kanfiszer et al., 2017), but the extent of gender differences is unclear. Women also reported experiences of sexual victimisation due to difficulties with social cues and assertiveness (Bargiela et al., 2016; Kanfiszer et al., 2017). Autistic women in the Kanfiszer et al. (2017) study expressed a disconnection with female gender identity and rejection of feminine gender roles, which alienated them from non-autistic female peers.
Psychosocial characteristics
Mainly using data from diagnostic services, 25 studies discussed the psychological and social characteristics of individuals diagnosed with autism in adulthood, including autistic traits, cognitive ability, personality and social functioning. Notably, a diagnostic service in Japan reported a wide range of findings on autistic traits, personality and cognitive ability in their clients (Kanai et al., 2012; Kanai, Iwanami, Hashimoto, et al., 2011; Kanai, Iwanami, Ota, et al., 2011; Tani et al., 2012). The quality appraisal scores for this group of studies varied greatly (range = 0.89–2.00), with lack of attention to potential confounding factors as the most common methodological flaw. The majority of studies involved male-majority samples (n = 19) and excluded adults with intellectual disability (n = 13). Twelve studies provided data on co-occurring conditions other than intellectual disability.
Autistic traits
Several studies used self-report measures including the Autism Quotient (AQ), Empathy Quotient (EQ) and Systemising Quotient (SQ), as well as informant report and clinician assessment to evaluate autistic traits in participants. Adulthood-diagnosed participants’ high AQ and low EQ scores indicated a high level of autistic traits and difficulties in social understanding (Abbott et al., 2018; Kanai, Iwanami, Ota, et al., 2011; Russ et al., 2018). Autistic adults without intellectual disability tended to exhibit traits related to social interaction difficulties to a greater extent than restrictive/repetitive behaviours and interests (Crucitti et al., 2018; Hofvander et al., 2009; Kanai, Iwanami, Ota, et al., 2011), and language difficulties were relatively uncommon (Hofvander et al., 2009). Consistent with quantitative findings on social difficulties, participants from qualitative studies spoke of negative social experiences and attempts to emulate acceptable social behaviour (e.g. Bargiela et al., 2016; Hickey et al., 2018; Kanfiszer et al., 2017). A small study using the Rorschach Inkblot Test reported that participants’ responses reflect cognitive inflexibility and poor social adaptation (Crucitti et al., 2018), though the validity of the Rorschach Inkblot Test in examining autistic traits has not been evaluated. Adults also reported sensory sensitivities that may increase stress in certain situations (R. S. Smith & Sharp, 2013). Although some autistic traits were also present in non-autistic adults with intellectual disability, autistic adults with intellectual disability were more likely to display social avoidance, routines and repetitive behaviours (e.g. Beighley et al., 2014; Bhaumik et al., 2010; Matson & Dempsey, 2008). Although adulthood-diagnosed individuals displayed a range of autistic traits, social interaction difficulties were the most frequent in this population (e.g. Hofvander et al., 2009).
Cognitive ability
There is uncertainty on whether intelligence, executive function and memory in adulthood-diagnosed individuals without intellectual disability differ from the general population. The full-scale IQ of autistic adults tended to be average or slightly above average (e.g. Kanai et al., 2012; Lehnhardt et al., 2016; Nydén et al., 2010). Diagnostic service data showed although whether the adult received an autism spectrum diagnosis was unrelated to IQ (Happé et al., 2016), adults receiving an Asperger’s Syndrome diagnosis had higher IQ than adults diagnosed with other subtypes (Kanai et al., 2012). Although some adults reported executive function difficulties (Baldwin & Costley, 2016; Davids et al., 2016), there were conflicting findings on how autistic adults’ executive function abilities compare to standardised norms (Abbott et al., 2018; Davids et al., 2016; Lehnhardt et al., 2016; Nydén et al., 2010). Although autistic adults performed well in primary memory tests, there were difficulties with other memory tasks involving visual and auditory information (Nydén et al., 2010).
Personality
Individuals receiving a diagnosis in adulthood tended to display personality characteristics related to emotional instability, introversion and social detachment on self-report measures evaluating various personality traits (Kanai, Iwanami, Hashimoto, et al., 2011; Kanai, Iwanami, Ota, et al., 2011; E. Rydén & Bejerot, 2008). High scores on neuroticism, psychoticism, stress-susceptibility and embitterment showed a tendency towards negative emotional states. Low extraversion and agreeableness, high detachment and lack of assertiveness revealed a propensity for aloneness and social avoidance.
Education, employment and functioning
Adulthood-diagnosed individuals without intellectual disability tended to experience difficulties in employment, independent living and other aspects of functioning. Over half of autistic adults from diagnostic services completed high school, and a significant proportion attended university (Happé et al., 2016; Hofvander et al., 2009). However, the autistic adults identified by Brugha et al.’s (2011) epidemiological study were less educated, suggesting a discrepancy between adults attending diagnostic services and yet-undiagnosed adults in the community. Over half of autistic adults were not employed at the time of diagnosis (Happé et al., 2016; Hofvander et al., 2009; E. Rydén & Bejerot, 2008), in line with self-reported difficulties in the workplace (Baldwin & Costley, 2016; Griffith et al., 2012). Studies using diagnostic service data reported that between 30% and 40% of autistic adults receiving a first-time diagnosis lived with parents or in supported accommodation (Hofvander et al., 2009; Lehnhardt et al., 2016). Marriage et al. (2009) found that individuals diagnosed in adulthood outperformed adults diagnosed in childhood in the ‘education’ and ‘independence’ domains of adulthood functioning, though age differences between groups may have influenced outcomes. Consistent with low rates of employment and independent living, E. Rydén and Bejerot (2008) reported adults who received an autism diagnosis scored less well on the Global Assessment of Functioning (GAF) than those assessed but not diagnosed. Interestingly, adults self-evaluated as more competent than clinician evaluations on the GAF (E. Rydén & Bejerot, 2008), suggesting a discrepancy between adults’ and clinicians’ standards for optimal functioning. A diagnostic service reported that 83% of autistic adults were single at the time of diagnosis (E. Rydén & Bejerot, 2008), and the proportion who have ever had an intimate relationship varied from ‘a few’ (Hofvander et al., 2009, p. 8) to over 50% (Happé et al., 2016).
Co-occurring conditions
Thirty-six studies examined co-occurring mental health, neurodevelopmental and neurological conditions. No studies examined non-neurological physical health conditions. Some studies examined co-occurring conditions among individuals receiving an autism diagnosis, typically from diagnostic services (e.g. Hofvander et al., 2009), while others aimed to identify and diagnose autism in adults with another condition (e.g. Berkvens et al., 2015; Takara & Kondo, 2014). Most studies involved male-majority samples (n = 26). Fourteen studies specified inclusion of adults with intellectual disability. Studies in this theme overlapped considerably with the ‘Psychosocial factors’ theme, with similar variation in quality appraisal scores (range = 0.89–2.0) and potential confounding factors as the most frequent methodological problem. In addition, prevalence studies tended to suffer from inadequate samples due to recruiting all participants from the same service.
Mental health
Mental ill-health is common among adults receiving an autism diagnosis (e.g. Hofvander et al., 2009; Tani et al., 2012). Studies most commonly discussed depression, anxiety and psychotic disorders, comparing autistic adults with the general population (e.g. Cassidy et al., 2014; Kanai, Iwanami, Hashimoto, et al., 2011) and/or adults who were assessed but not diagnosed with autism (e.g. Happé et al., 2016; Wilson et al., 2016).
Depression (13%–50%) and anxiety (10%–50%) were highly prevalent among adults undergoing autism assessment regardless of diagnostic outcome (e.g. Geurts & Jansen, 2012; Happé et al., 2016). Autistic adults self-reported high levels of depression and anxiety (Lehnhardt et al., 2016; Powell & Acker, 2016) even in the absence of a formal mental health diagnosis (Kanai, Iwanami, Hashimoto, et al., 2011). A small case-control study found overlaps between autistic traits and social anxiety symptoms (Cath et al., 2008). Prichard et al. (2010) reported a patient whose anxiety disorder diagnosis was changed to Autistic Disorder following treatment. Marriage et al. (2009) found that depression was more prevalent among the adulthood-diagnosed sample compared to childhood-diagnosed adults, though anxiety disorders were similarly prevalent. As undiagnosed autistic adults often seek treatment for mental health difficulties such as depression (Bargiela et al., 2016; Geurts & Jansen, 2012; Lehnhardt et al., 2016), identifying predictors of autism diagnosis in depressed adults such as interpersonal friction and bullying (Takara & Kondo, 2014) may help to recognise those needing assessment. In line with high depression prevalence, suicidal ideation (66%) and suicidal behaviour (35%) were also common among autistic adults (Cassidy et al., 2014).
Studies exploring the co-occurrence of autism and psychosis typically involved populations receiving psychiatric treatment (e.g. Mandell et al., 2012), though several examined adults from autism diagnostic services (e.g. Geurts & Jansen, 2012; Russell et al., 2016). Schizophrenia is a common concurrent diagnosis in adult psychiatric patients found to meet autism criteria (Mandell et al., 2012; Raja & Azzoni, 2010; Unenge Hallerback et al., 2012). Davidson et al. (2014) reported a 3.6% autism prevalence in a mixed adolescent-adult sample of people with first-episode psychosis. Meera Roy and Balaratnasingam (2010) identified 12 autistic Indigenous Australian adults who were previously misdiagnosed with schizophrenia at a remote area mental health service. Studies from autism diagnostic services estimated psychotic disorder prevalence to be 2.1%–12% among their clients (Geurts & Jansen, 2012; Hofvander et al., 2009; Marriage et al., 2009; Nylander et al., 2013; Russell et al., 2016). In case reports and screening studies, adults presenting with psychotic symptoms had developmental histories and psychosocial characteristics that led to autism diagnosis (Arora et al., 2011; Davidson et al., 2014; Meera Roy & Balaratnasingam, 2010).
Other studies discussed mental illnesses including OCD, eating disorders and PDs. OCD and autism share similar traits (Cath et al., 2008) and co-occur frequently in autistic adults (e.g. Cath et al., 2008; Hofvander et al., 2009; Nahar et al., 2018; Wikramanayake et al., 2018). Two studies from autism diagnostic services reported 5% (Hofvander et al., 2009) and 13.2% (E. Rydén & Bejerot, 2008) of their clients had an eating disorder. Although only 15% of autistic adults carried a previous PD diagnosis at time of assessment (Geurts & Jansen, 2012; Nylander et al., 2013), they self-reported high levels of PD traits (Kanai, Iwanami, Ota, et al., 2011; E. Rydén & Bejerot, 2008). Sixty-two percent of autistic adults met criteria for at least one PD, primarily obsessive-compulsive (32%), avoidant (25%) and schizoid PDs (21%) (Hofvander et al., 2009). As autistic traits overlap with aspects of several PDs, the categorical model of PDs may have limited validity in autistic adults (Hofvander et al., 2009).
Attention-deficit hyperactivity disorder
Attention-deficit hyperactivity disorder (ADHD) occurs frequently in adulthood-diagnosed individuals, with inattentive and combined types more common than the hyperactive type (Hofvander et al., 2009; Mandy Roy et al., 2013; Nydén et al., 2010). Mandy Roy et al. (2013) identified previously undiagnosed Asperger’s Syndrome in 8 of 53 (15.1%) adults receiving first-time diagnosis of ADHD, suggesting that both conditions may be under-recognised in adults. Adults with both conditions did not differ from autism or ADHD-only groups on neurocognitive measures (Nydén et al., 2010).
Intellectual disability
Prevalence of autism in populations with moderate-to-profound intellectual disability was high (21% to 42.3%) (Brugha et al., 2016; Saemundsen et al., 2010), including some cases of first diagnosis in adulthood (Saemundsen et al., 2010). Although the ‘lost generation’ includes adults with intellectual disability, these adults have not been adequately included in studies on adulthood autism diagnosis. Most studies tended to exclude these individuals (e.g. Bargiela et al., 2016; Hofvander et al., 2009; Kanai, Iwanami, Hashimoto, et al., 2011). Individuals with intellectual disability accounted for 4%–38% of participants in studies that included them (Geurts & Jansen, 2012; Happé et al., 2016; Nylander et al., 2013; Rutherford, McKenzie, Johnson, et al., 2016; Wilson et al., 2016). Several studies recruited participants with intellectual disability from the same developmental centres in South-Eastern United States (Matson & Dempsey, 2008; Matson, Wilkins, & Ancona, 2008; Matson, Wilkins, Smith, & Ancona, 2008). Studies of autism in adults with intellectual disability tended to be of low-to-moderate quality, with failure to consider confounds and reduced validity and reliability in screening and assessment methods (e.g. using a symptom checklist rather than validated assessment tools to determine diagnostic status; Matson et al., 2012; Matson, Wilkins, & Ancona, 2008) as the most common problems. As communication difficulties are common in adults with intellectual disability, researchers often relied on informant report of observed behaviour (e.g. Matson & Dempsey, 2008) to assess this population.
Other conditions
Other neurological and neurodevelopmental conditions have been found to co-occur with autism in adults. Adults with Dravet syndrome (Berkvens et al., 2015) and agenesis of the corpus callosum (Paul et al., 2014) had higher autism prevalence than the general population. Preliminary evidence from longitudinal studies suggests an overlap between developmental language disorder (DLD) and autism, as people diagnosed with DLDs in childhood have a higher rate (2.1%) of receiving an autism diagnosis in adolescence and adulthood (Mouridsen & Hauschild, 2009), and 34% of a sample of 38 adults with DLD diagnoses were found to meet autism criteria (Bishop et al., 2008).
Experiences of diagnosis
A total of 17 mostly qualitative studies described the experience of receiving an autism diagnosis in adulthood and explored the emotional impact and meanings ascribed to diagnosis. Research conducted in the United Kingdom dominates this topic area (see Bargiela et al., 2016; Hickey et al., 2018; Raymond-Barker et al., 2018), though a US-based project collected online survey data from autistic adults and their partners around the world (Lewis, 2016a, 2016b, 2017a, 2017b). Most studies (n = 15) focused on the first-person experiences of adults while two focused on mothers (Raymond-Barker et al., 2018) and partners (Lewis, 2017b), respectively. Study samples varied in gender distribution, with male-majority (n = 5), equal-gender (n = 6) and female-majority (n = 4) samples. Three studies focused on women (Baldwin & Costley, 2016; Bargiela et al., 2016; Kanfiszer et al., 2017), while two studies examined middle-aged (Griffith et al., 2012) and older adults (Hickey et al., 2018), respectively. Only one study included adults with intellectual disability (Kanfiszer et al., 2017). Two studies reported data on co-occurring conditions other than intellectual disability within the sample (Baldwin & Costley, 2016; Powell & Acker, 2016), and two more studies provided scores from self-report depression and anxiety questionnaires (Bargiela et al., 2016; Hickey et al., 2018). Studies tended to be of moderate-to-high quality (range = 1.40–1.78), but few qualitative studies were able to critically reflect on the relationship between researcher and participant as recommended by CASP (2018).
Adults frequently described lifelong feelings of being different from peers, social isolation and bullying prior to diagnosis (Hickey et al., 2018; Lewis, 2016b; Punshon et al., 2009). Over 50% of adults in a UK survey had expected the diagnosis (Jones et al., 2014), but others described it as a surprise (Crane et al., 2018). Adults generally expressed relief and happiness that their concerns were validated (Jones et al., 2014; Lewis, 2016b, 2017b; Punshon et al., 2009), but also described negative reactions such as shock, anger or confusion (Bargiela et al., 2016; Jones et al., 2014; Lewis, 2016b; Powell & Acker, 2016). Autistic adults expressed that the diagnosis gave them a new framework to interpret their experiences (e.g. Bertilsdotter Rosqvist, 2012; Lewis, 2016b; Powell & Acker, 2016), which promoted self-acceptance and diminished guilt and inadequacy (Lewis, 2016b; Punshon et al., 2009; Tan, 2018). Some autistic adults asserted that autism is a positive intrinsic difference (e.g. Lewis, 2016b; Tan, 2018), but others viewed autism more negatively and separated it from their identities (Griffith et al., 2012; Hickey et al., 2018). In many cases, improved self-understanding after diagnosis helped adults develop useful strategies in everyday life (Hickey et al., 2018; Kanfiszer et al., 2017; Lewis, 2016b; Tan, 2018). The formation of autistic self-identity was facilitated by meeting autistic peers, building upon self-understanding through comparisons (Bargiela et al., 2016; Hickey et al., 2018; Lewis, 2016b; Punshon et al., 2009; Tan, 2018). Interestingly, self-diagnosed adults reported similar experiences, where adopting an autistic label gave them feelings of relief, self-understanding and access to online autistic communities (Lewis, 2016a).
Post-diagnosis support
Lack of clear pathways to formal support after diagnosis was well-documented from the perspectives of autistic adults, families and service providers (e.g. Crane et al., 2018; Griffith et al., 2012; Lewis, 2017b; Raymond-Barker et al., 2018). A UK survey found that autistic adults’ preferred forms of support were counselling (44.5%), social skills training (36.7%) and support groups (35.9%) (Jones et al., 2014). Although some autistic adults described accessing occupational adjustments and services due to their diagnosis (Powell & Acker, 2016), almost half of the adults in another study were offered no post-diagnosis support (Jones et al., 2014). Some autistic adults found existing autism services unsuitable as they mostly targeted children or adults with high support needs (Crane et al., 2018). Mothers of adults described the need to actively pursue potential sources of support (Raymond-Barker et al., 2018). Diagnosticians were often unable to provide follow-up due to pressure and lack of resources (Crane et al., 2018), leaving clients dissatisfied with the conclusion of their diagnosis experience (Jones et al., 2014).
Potential sources of informal support include family, friends, partners and other autistic adults. Mothers involved in their adult children’s diagnosis expressed positive reactions to the diagnosis (Raymond-Barker et al., 2018), but autistic adults described both positive and negative reactions from their parents (Crane et al., 2018; Punshon et al., 2009). In a survey of mostly female married partners of late-diagnosed adults, the partners reported initial reactions of anger and hopelessness when learning the diagnosis, before accepting and supporting their autistic partner (Lewis, 2017b). Adults expressed that even when families were accepting, misconceptions about autism made support difficult (Crane et al., 2018; Punshon et al., 2009). In contrast, adults described interactions with other autistic adults as validating and fulfilling (Bargiela et al., 2016; Hickey et al., 2018; Tan, 2018), where their differences were normalised (Bargiela et al., 2016; Hickey et al., 2018; Tan, 2018). The gap in formal support means that social relationships become important sources of support for adults, with support from autistic peers viewed as especially valuable.
Discussion
Research in adult autism diagnosis expanded alongside increased autism awareness and prevalence statistics (Lyall et al., 2017; Nylander et al., 2013), with a growing number of studies that encompass diverse methodologies and areas of interest. Methodologically, there is a dominance of retrospective studies using diagnostic service data to examine sample characteristics and diagnostic processes (e.g. Happé et al., 2016). Thematically, the overlap between autism and other conditions is the most prominent, encompassing both autism-specific and mainstream psychiatry contexts. Although earlier studies relied on clinical records (Ghaziuddin & Zafar, 2008; E. Rydén & Bejerot, 2008), there has been a growth in studies using self-report methods (e.g. Crane et al., 2018; Hickey et al., 2018; Tan, 2018). This suggests the experiential knowledge of autistic adults is increasingly valued by researchers, adding a new perspective to research on adult autism diagnosis.
Longitudinal prevalence studies showed an increase in diagnosed autism among adults in more recent years (e.g. Jensen et al., 2014), which may be explained by a combination of adult diagnosis and childhood-diagnosed individuals entering adulthood. The implementation of DSM-IV after 1994 has also been reflected in increased first-time adult diagnoses (Nylander et al., 2013). Lower prevalence in older adult age groups (e.g. Bachmann et al., 2018; Jensen et al., 2014) may reflect increased use of camouflaging strategies or reduced autism knowledge and opportunities for detection with increasing age.
Findings on referral and assessment pathways suggested that referring professionals’ lack of autism knowledge was detrimental to adults and diagnosing professionals, resulting in delayed detection (Geurts & Jansen, 2012; Jones et al., 2014), mistrust of health professionals (Lewis, 2017a) and inappropriate referrals (Rutherford, McKenzie, Forsyth, et al., 2016). Although research so far indicated that fewer adults met DSM-5 ASD criteria compared to previous versions (e.g. Young & Rodi, 2014), it remains to be seen whether the change would influence the incidence of adult autism diagnosis over time.
Studies have highlighted a discrepancy between self-reported and clinician-assessed autistic traits in adulthood-diagnosed women (Happé et al., 2016; Wilson et al., 2016). A potential explanation is that clinical measures are insufficiently sensitive to the presentation of autistic traits in women (Wilson et al., 2016), especially considering women’s reported use of camouflaging strategies (Bargiela et al., 2016). Another consideration is that women experience heightened social demands from increased involvement in relationships (Lehnhardt et al., 2016), which may lead to increased awareness of their own difficulties. It would be useful for clinicians working with women to be sensitive to atypical presentations of autistic traits and consider the interaction between individual capabilities and social demands in making recommendations for diagnosis and support.
The interrelationships between autistic traits, personality and co-occurring mental illness add complexity to measuring psychosocial characteristics of adulthood-diagnosed individuals. Personality traits relating to introversion and neuroticism may potentially reflect social difficulties and patterns of rigid thinking in autism as well as depressive and anxious symptoms. The similarity between repetitive behavioural tendencies and symptoms of anxiety and OCD (Cath et al., 2008; Wikramanayake et al., 2018) may also contribute to misdiagnosis and ineffective treatment. As common co-occurring conditions like depression and ADHD are known to negatively affect cognitive function (McDermott & Ebmeier, 2009; Nydén et al., 2010), it is challenging for researchers to disentangle autism’s relationship with cognitive abilities while using samples representative of the autistic adult population.
Study participants were predominantly men with average-to-high intellectual ability who were unmarried, well-educated, not employed, with history of depression and/or anxiety. While this profile may reflect the underlying characteristics of the late-diagnosed autistic adult population, the characteristics of diagnostic services contributing data to these studies may have resulted in sample bias. Lewis (2017a) identified barriers that disproportionately prevent women and those from low socioeconomic backgrounds from accessing autism assessment. Prevalence studies also detected previously unidentified autistic adults in the community (Brugha et al., 2011) and among populations with mental illnesses (Mandell et al., 2012). As autistic traits may present similarly to mental illness symptoms, co-occurring mental disorders may act as a barrier to autism diagnosis due to complexities of differential diagnosis (Lai & Baron-Cohen, 2015; Lehnhardt et al., 2013). Differential diagnosis is particularly difficult in adults with intellectual disability who may have difficulty describing their internal experiences, leading to their behaviours being misattributed to intellectual disability or schizophrenia (Meera Roy & Balaratnasingam, 2010). However, experience with mental health treatment could potentially improve access by increasing individuals and carers’ knowledge of psychiatric services that provide autism assessment. Mental health treatment also offers an opportunity for clinicians to recognise and refer clients for adult autism assessment (Geurts & Jansen, 2012; Takara & Kondo, 2014). Furthermore, inconsistencies in the reporting of demographics and co-occurring conditions across different studies makes disentangling the influence of demographic and health factors on diagnosis more challenging.
Considering the complex mental health needs of individuals diagnosed in adulthood (Geurts & Jansen, 2012; Hofvander et al., 2009) and emotional reactions following diagnosis (Jones et al., 2014; Lewis, 2016b), the lack of formal support after diagnosis is of concern. As diagnostic services often do not provide ongoing support (Crane et al., 2018), a collaborative multidisciplinary effort is needed to create support pathways after diagnosis. Services aimed at improving social skills and supporting social inclusion are highly desired by adults (Baldwin & Costley, 2016; Jones et al., 2014), with social interaction difficulties being the most common autistic trait in this population (Hofvander et al., 2009; Kanai, Iwanami, Ota, et al., 2011). As autistic adults often have difficulties with employment (e.g. Griffith et al., 2012; Marriage et al., 2009), training employers on supporting autistic adults’ occupational needs may also be beneficial. Adults who were assessed but not diagnosed with autism would also benefit from counselling and mental health support due to high rates of mental illness (Geurts & Jansen, 2012; E. Rydén & Bejerot, 2008) and reported negative reactions following assessment (Powell & Acker, 2016). As some adults emphasised that they view autism as a positive part of their identities (Lewis, 2016b; Tan, 2018), it is important for service providers to recognise and value autistic adults’ strengths while supporting them in areas of difficulty.
Limitations
This scoping review did not include grey literature and reviews in this research area. A more comprehensive scoping review may have been able to contrast and synthesise information from a wider variety of sources including government guidelines and professional opinion.
Unlike a conventional systematic review, the scoping review did not exclude studies based on methodological rigour, nor was it able to discuss each theme in great detail. A follow-up systematic review narrowly focused on distinct themes would produce a more in-depth account of the literature using only high-quality evidence.
The authors were also unable to consult with stakeholder representatives as optionally recommended by Arksey and O’Malley (2005). A scoping review incorporating insight from autistic adults, carers and diagnosticians would provide researchers with an additional source of relevant literature and inform the development of themes using real-life experience.
Future directions
UK studies dominate research on adulthood autism diagnosis. Disparities in culture, autism awareness and healthcare access in different countries have important implications for autism diagnosis. Further research in non-UK and non-Western countries would allow future researchers to analyse the effect of national healthcare systems on adult autism diagnosis and inform government policy.
Studies mainly using proposed criteria and retrospective analysis found that compared to previous versions, the DSM-5 ASD criteria applied to a smaller number of adults with stronger tendencies towards restrictive interests and repetitive behaviours (e.g. Beighley et al., 2014; Wilson et al., 2013). However, the application of the current DSM-5 criteria, which specifies that required autism traits may be met currently or by history, has not yet been evaluated in adult diagnostic practice. As the use of DSM-5 becomes more widespread, there is an opportunity for researchers to evaluate the effect of DSM-5 criteria on rates of adult autism diagnosis in real-life settings.
A gap exists in high-quality research about experiences and needs of adults with intellectual disability receiving an autism diagnosis. Despite the frequent co-occurrence of autism and intellectual disability in adults (Brugha et al., 2016; Saemundsen et al., 2010), only a small proportion of studies intentionally included these individuals. Adapting qualitative methods for verbal adults with intellectual disability could help enrich research into diagnosis experiences. As adults with intellectual disability may be unable to voluntarily seek diagnosis, examining the pathways to diagnosis for these individuals would help improve recognition. As autistic adults with intellectual disability have different needs from non-autistic adults with intellectual disability (Matson & Dempsey, 2008; Matson et al., 2009), improved recognition would inform provision of tailored support.
Although adulthood-diagnosed individuals often wished they were diagnosed earlier (Baldwin & Costley, 2016; Lewis, 2016b; Powell & Acker, 2016), only one study compared adults diagnosed at different ages (Marriage et al., 2009). Adults who grew up with an autism diagnosis may differ in experiences, psychosocial outcomes and autism beliefs from adults receiving a diagnosis. Understanding the distinct needs of adults diagnosed at each developmental stage would help inform development of specialised support programmes.
Many adults participated in autistic peer communities following autism diagnosis (Hickey et al., 2018; Lewis, 2016b; Tan, 2018). In-depth research into functions of peer support, characteristics of online communities and comparing support from autistic versus non-autistic people could inform collaborative development of formal peer support services by autistic adults, services and organisations.
This review also highlighted other potential areas for future research, such as cognitive differences between autistic and non-autistic adults, transgender and non-binary genders, symptom overlap between autism and related psychiatric conditions, and the relationship between autistic traits and personality dimensions.
This scoping review identified important areas for future research on autism in adulthood. It offers a starting point for enabling positive experiences across diagnostic services, disability organisations, adults and their supporters using current knowledge. It is important that the healthcare community is equipped for the needs of the ‘lost generation’ as more adults seek explanation for their lifelong differences.
Supplemental Material
Appendix_A-_Search_strategy_for_all_databases – Supplemental material for Diagnosis of autism in adulthood: A scoping review
Supplemental material, Appendix_A-_Search_strategy_for_all_databases for Diagnosis of autism in adulthood: A scoping review by Yunhe Huang, Samuel RC Arnold, Kitty-Rose Foley and Julian N Trollor in Autism
Supplemental Material
Appendix_B-_Example_strategy_for_Medline_database_search – Supplemental material for Diagnosis of autism in adulthood: A scoping review
Supplemental material, Appendix_B-_Example_strategy_for_Medline_database_search for Diagnosis of autism in adulthood: A scoping review by Yunhe Huang, Samuel RC Arnold, Kitty-Rose Foley and Julian N Trollor in Autism
Supplemental Material
Appendix_C-_List_of_included_articles-_revised – Supplemental material for Diagnosis of autism in adulthood: A scoping review
Supplemental material, Appendix_C-_List_of_included_articles-_revised for Diagnosis of autism in adulthood: A scoping review by Yunhe Huang, Samuel RC Arnold, Kitty-Rose Foley and Julian N Trollor in Autism
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Cooperative Research Centre for Living with Autism (Autism CRC), established and supported under the Australian Government’s Cooperative Research Centres Program. The authors also acknowledge the financial support of the Australian Government Research Training Program.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.