
Abstract
Introduction
For many patients, audio-visual appointments have provided a timely and efficient way of seeking advice, assessment and treatment for their hand injuries during the NHS response to COVID-19. This study aimed to explore the experience of hand units across the UK in determining the safe and judicious use of audio-visual outpatient care for the management of acute upper limb trauma.
Methods
An online cross-sectional survey was sent to the therapy leads of hand units across the UK. Questions focused on the experience of using audio-visual technology in the management of upper limb trauma, and the relevant factors in determining its appropriate use. A deductive mixed methods analysis was used to identify both common themes and capture community experience and characteristics.
Results
A total of 51 out of 76 hand therapy units completed the survey; a response rate of 67%. Of these, 82% (42/51) reported using audio-visual technology to manage upper limb trauma during the UK COVID-19 lockdown. When determining patient suitability for audio-visual consultations, 73% (37/51) of respondents reported the use of COVID-19 guidelines, but only 35% (18/51) reported the use of a clinical decision-making tool. In agreement with our experience at Salisbury Hospital Foundation Trust, 92% (47/51) had concerns relating to the use of audio-visual care.
Conclusion
The choice of safely managed remote care or in-person consultation has, to date, largely relied on the discretion of the clinician. A carefully designed clinical decision-making tool for the management of upper limb trauma is needed for use both in clinical practice and in future service planning.
Introduction
Digital transformation is an essential component of the NHS Five year forward view 1 and the NHS Long Term Plan. 2 Critical priorities include the development of digital technologies, innovative delivery of care, and improvement of remote consultation for assessment and treatment. As part of the ‘Digital First’ agenda, the United Kingdom (UK) Government has proposed that technology-enabled care be used to ‘engage with the widest cohort possible, through new ways of working, to achieve greater reach and to minimise avoidable deterioration’. 3
The COVID-19 pandemic has inspired a rapid adoption of new ways of working. 4 The use of digital technology has been promoted as part of this ‘Digital First’ approach, which is designed to minimise disease transmission and protect both patients and staff. 3 During Phase One of the UK response to COVID-19 (January-May 2020), UK Government advice stated that ‘as far as practicable, video or telephone appointments should be offered by default for all outpatient activity without a procedure, unless there are clinical or patient choice reasons to change and replace with in-person contact’. 5
During the height of the pandemic, upper limb trauma caseloads were impacted by a 37% reduction in emergency activity recorded in healthcare settings. This sharp reduction was in part attributed to a change in healthcare seeking behaviour and the availability of alternative access in the form of online consultations.5–7 For upper limb trauma teams, this resulted in the rapid upscaling of new, technology-enabled service delivery options.4,8
A recent combined statement by the UK Chief Allied Health Professions Officers revealed that digital technology, including audio-visual consultation, will form part of the NHS collective strategic priorities for rehabilitation and recovery during the remainder of the COVID-19 response and beyond. 7 Audio-visual consultation is defined as a clinical interaction between the patient and health professional using both a video screen and microphone to communicate. This consultation could take place using a computer or smart device such as a phone or tablet.
For many patients, audio-visual consultation offered a safe and timely way to access advice, assessment and treatment of hand injuries during a period of national lockdown. As an early adopter of consultation, the Salisbury District Hospital hand therapy team conducted 739 consultations for upper limb trauma patients during Phase One of the UK response to COVID-19. However, subsets of patients were identified as requiring at least one in-person review in order to optimise clinical outcome. 8 Building on these observations, the decision was made to pilot a clinical decision-making tool to support staff to determine either remote or in-person care. The tool was developed and successfully implemented at pace in April 2020. It was designed to complement both COVID-19 exclusion factors5,9 and professional guidelines.10,11 The clinical criteria of patient-specific considerations included injury severity, social risk factors and mental health considerations (see Tables 1 and 2). At each appointment, the decision to continue with the model of care was reviewed with the patient to ensure that the care plan remained in the best interest of the patient.
Outpatient audio-visual use screening tool.
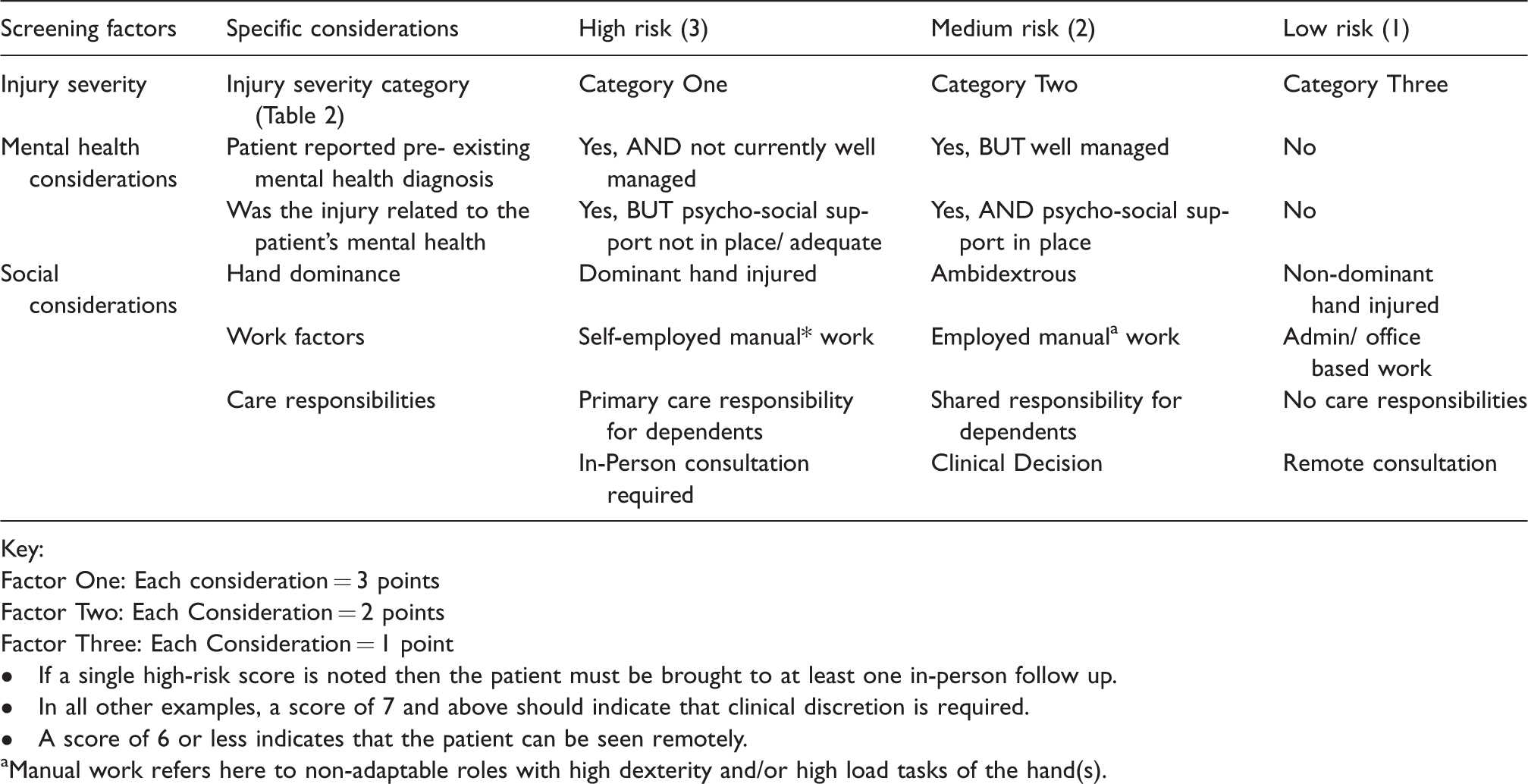
Key:
Factor One: Each consideration = 3 points
Factor Two: Each Consideration = 2 points
Factor Three: Each Consideration = 1 point
• If a single high-risk score is noted then the patient must be brought to at least one in-person follow up.
• In all other examples, a score of 7 and above should indicate that clinical discretion is required.
• A score of 6 or less indicates that the patient can be seen remotely.
aManual work refers here to non-adaptable roles with high dexterity and/or high load tasks of the hand(s).
Injury Severity Category for acute upper limb trauma/hand therapy follow up.
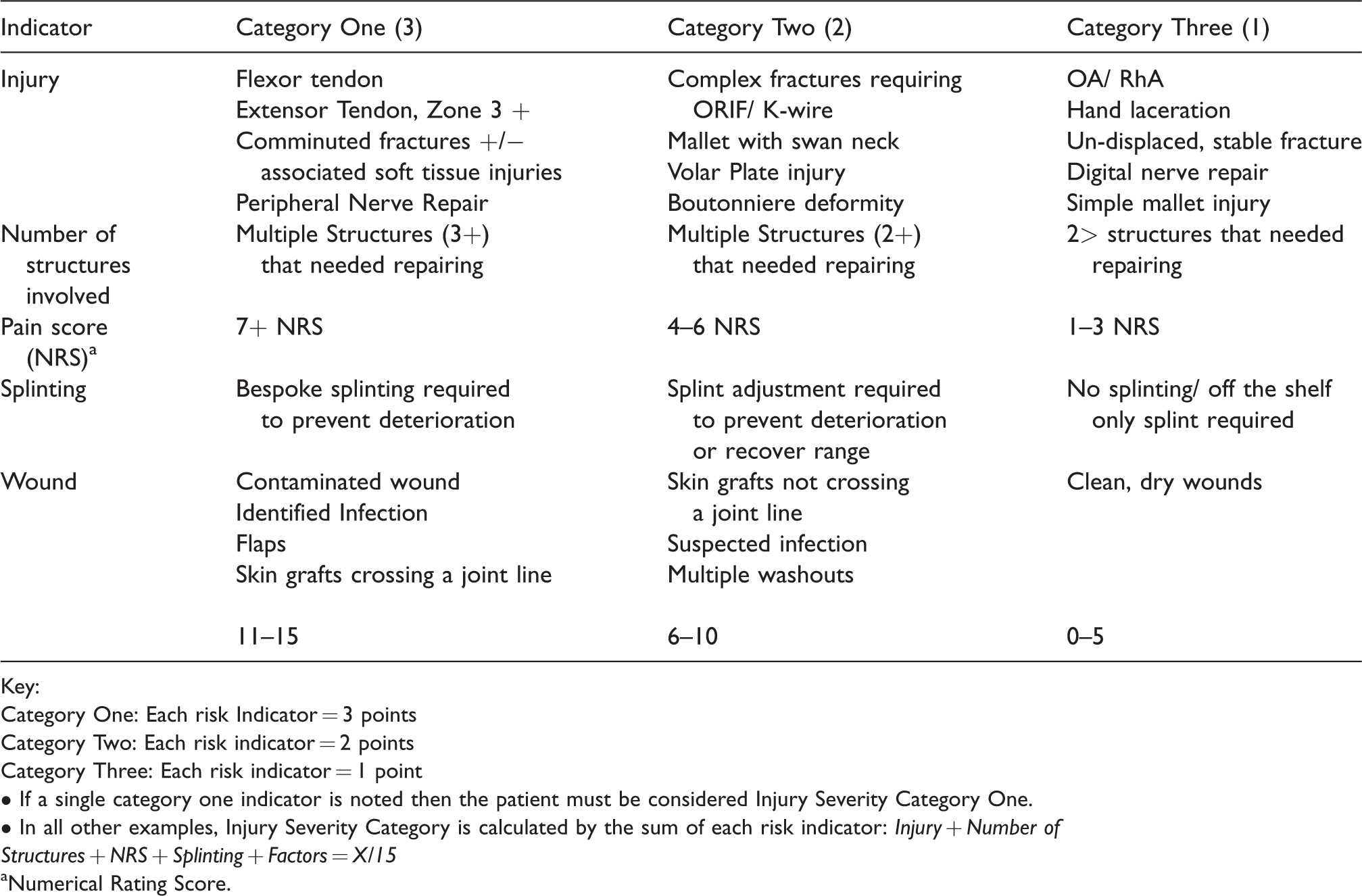
Key:
Category One: Each risk Indicator = 3 points
Category Two: Each risk indicator = 2 points
Category Three: Each risk indicator = 1 point
• If a single category one indicator is noted then the patient must be considered Injury Severity Category One.
• In all other examples, Injury Severity Category is calculated by the sum of each risk indicator: Injury + Number of Structures + NRS + Splinting + Factors = X/15
aNumerical Rating Score.
As NHS organisations work to reinstate critical services across the country, urgent and time-critical care is anticipated to return to, and surpass, pre COVID-19 levels due to the reactivation of delayed activities.6,7 It is therefore important to understand where audio-visual consultation services can be retained to benefit both patients and staff, and where clinical decision-making processes around the use of technology-enabled, remote care need to be further developed. During Phase Two of the COVID-19 response and beyond, proactive determination of either remote or in-person care to recover function post-injury will be essential to the success of urgent and elective hand surgery.
In order to understand the challenges and successes of implementing technology-enabled care, a national survey of practice was designed and conducted across hand units in the UK. The focus of the survey was the experience of using audio-visual technology in the management of acute upper limb trauma, and the relevant factors in determining its appropriate use. The aim of this study was to explore the experience of hand units across the UK in determining the safe and judicious use of audio-visual outpatient care in the management of acute upper limb trauma. Study findings will be used to inform future guidance and the need for a standardised clinical decision-making tool to optimise patient outcomes and support clinical staff.
Methods
Study design
An anonymised cross-sectional survey was sent to the therapy leads of hand units across the UK. A deductive mixed methods analysis was used to identify both common themes and capture community experience and characteristics.
Sampling
The study targeted hand therapy service leads due to their position and knowledge; in addition to the timely need to collect data. No single list of hand units existed, therefore the British Association of Hand Therapy (BAHT), British Society of Surgery of the Hand (BSSH) and Reconstructive Surgery Trials Network (RSTN) were approached and the data triangulated. Where gaps existed, follow-up calls were made to services managing upper limb injury to invite participation and strengthen secondary snowball sampling. This was complemented by a social media information campaign within the hand surgery community and peers to maximize recruitment. Seventy-six units offering upper limb trauma services in the UK were identified.
Data collection
An anonymised cross-sectional survey was sent out electronically with the British Association of Hand Therapists (BAHT) Covid-19 Bulletin survey and via targeted email invitation. The data collection survey was open for three weeks from the date of the final recruitment email (15th June – 6th July 2020) with an automatic reminder email sent after ten days.
Survey
The customised web-based survey collected information about the respondents’ experience of delivering audio-visual and in-person care for upper limb trauma cases during the UK COVID-19 lockdown (23rd March 2020 – 10th May 2020). The initial survey questions were designed and reviewed by the authors as well as lay people to ensure relevance, logic and simplicity prior to dissemination. The survey was subsequently refined and piloted amongst four expert colleagues who were blinded to the study purpose. Finally, the survey was peer-reviewed and approved by the British Association of Hand Therapist (BAHT) Clinical Evidence Committee and colleagues at the Reconstructive Surgical Trials Network (RSTN). The final version was uploaded to an online survey tool (SurveyMonkey). The survey consisted of 19 questions organized into six sections (see appendix I, supplementary material). Respondents were presented with a series of closed multiple choice and checkboxes (n = 10) and open ended text questions (n = 9). The aim was to further explore each department’s experience of delivering services during Phase One of the UK’s response to COVID-19. They were also asked to complete questions about pre-existing services, the use of clinical decision-making tools to determine the type of appointment offered, and staff and patient feedback on the use of audio-visual equipment.
Data management and analysis
The data was collated onto an Excel spreadsheet. EM and MR completed the initial data clean. The data set was deductively analysed using a mixed methods approach. A combination of thematic and descriptive statistical analysis was used to determine themes and capture community experience and characteristics. Thematic analysis was performed by two evaluators (EM, MR) of different professions using a mixed coding approach. 12 Data were then classified and compared to create initial codes. Codes were grouped into themes and reviewed to ensure accurate reflection of the extracts and the broader data set. Triangulation and verification was undertaken by additional research team members in order to minimise bias . The final themes were refined and given definitions and labels to encompass the findings. Descriptive statistical analysis was applied to the data to detail the frequencies and levels of agreement for each statement.
Ethical considerations
All data was anonymised to minimise risk to respondents. The study was voluntary, easily accessible by an email link and took an average of 7 minutes to complete. It could be paused and resumed if data was not immediately available, minimizing disruption to the respondent. Ethical approval was sought but not required due to the lack of patient data, engagement or risk to those responding to the survey.
Results
A total of 51 hand units with an upper limb trauma caseload returned completed surveys; a response rate of 67% (51/76). Findings suggest that 82% (42/51) of responding hand units reported using audio-visual technology to manage upper limb trauma during the UK COVID-19 lockdown, with 16% (8/51) reporting pre-existing web-based services Of the units delivering audio-visual services, 92% (47/51) reported a delay in being able to offer the services due to a lack of available hardware and software technology. This delay ranged from 1 to 80 days to establish audio-visual services, with an average of 28 days. The number of new upper limb trauma cases per unit ranged from 1 to 650 with an average of 185 patients; 33% (17/51) of recorded trauma patients were seen using audio-visual methods.
The majority of respondents (73%, 37/51) reported the use of COVID-19 guidelines for determining patient suitability for technology-enabled consultations, but only 35% (18/51) used a clinical decision-making tool. In agreement with our experience at Salisbury Hospital Foundation Trust, 92% (47/51) had concerns with the use of technology-enabled remote care, either overall or for certain patients.
Thematic analysis allowed the grouping of the reasons for these concerns into four major themes: (i) access to clinical services, (ii) patient factors, (iii) mitigation of clinical risk, and (iv) the use of guidelines in decision-making when providing audio-visual services.
Access to clinical services
The rapid scaling-up of services meant that the majority (92%, 47/51) of participating services were unable to offer audio-visual consultations from the beginning of COVID-19 lockdown. Most common reasons cited were limited connectivity or quality of Wi-Fi access, and lack of availability of technology. ‘I did not have audiovisual technology available to me so most of my work has been using the phone only’. Respondent 38 ‘Technology provision not always available- fuzzy screens so could not see anything, cutting out/freezing’. Respondent 27 ‘Connection can be interrupted, camera quality varies for viewing structures, a patient's ability to verbally explain their symptoms might affect the decisions made’. Respondent 16
Patient factors
A variety of patient factors were noted by respondents to influence the successful use of audio-visual technology for assessment and treatment of upper limb injury.
Patient anxiety was the main mental health consideration raised by respondents (39%, 20/51). Anxiety regarding the outcome of the injury was reported to limit participation, as well as anxiety over the use of new technology, process and the perception that this was the only option being offered. Concern for patient psychological welfare extended to those who appeared to lack motivation or presented as isolated, depressed or withdrawn during audio-visual consultations and those with injuries directly linked to their mental health, i.e. deliberate self-harm. ‘Mental health issues- anxiety/depression, self-harm… Limited support systems at home to support progression’. Respondent 26
Respondents overall experience of patients' ability and desire to use audio-visual services varied between units. Where high risk patients e.g. mental health, vulnerable adults or children were unable to use audiovisual consultation, only 14% (7/51) of responding teams had the ability to complete home visits. This left concerns that a proportion of patients would remain unable to access essential care and services.
Mitigation of clinical risk
Injury severity, including complexity, location and mechanism of injury were highlighted as the most frequent reason for the need for in-person consultations by 96% (49/51) of respondents. Wound care, including post-operative management and infection risk, was cited as a high complication risk for remote consultation. The prevention of complications further included the need for manual treatment and bespoke splinting to manage pain conditions, stiffness, joint restriction and soft tissue contracture. Patients were reportedly offered in-person consultations at key intervals for treatment to mitigate for clinical risk and complication.
‘.(where) unable to deliver via video, e.g. needs a splint, mental health, cannot assess the problem- lag/contracture’. Respondent 33
Specific injuries were noted to progress more slowly and have poorer outcomes than expected by the team when seen remotely using audio-visual technology. These included high nerve lesions, isolated Flexor Pollicis Longus (FPL) tendon repairs and composite injuries that had resulted in the repair of more than one structure in the same anatomical area.
Whilst audio-visual technology ensured that upper limb trauma services were able to maintain their commitment to patients, staff reported concerns with the accuracy and reliability of performing assessment remotely. ‘Unable to comprehensively assess due to lack of hands on testing. Unable to view radiograph, MRI or CT from remote working’. Respondent 37 ‘Not able to complete all necessary tests; difficult with patients who have hearing or sight loss, learning difficulties, paeds.’ Respondent 15
‘I am unable to give full, quality care, without hands-on therapy’. Respondent 23
The ability of patients to follow instructions and for staff to be able to clearly demonstrate therapeutic techniques was inconsistent. Laterality issues and kinaesthesia were noted in a subset of patients when attempting to replicate positions and activities on screen. ‘Some patients don’t follow instructions well and cannot clearly capture movements on camera despite repeated advice. Assessment can be difficult or inaccurate’. Respondent 13
The use of guidelines in decision making when providing audio-visual services
Forty-seven percent (24/51) of the hand therapy units offering audio-visual consultation specifically stated the use of COVID-19 guidelines to be the primary decision-making tool for attendance. Government-led and published advice to shield vulnerable patients was followed. Essential attendance was only reported for patients with an absence of COVID-19 symptoms, risk factors or co-morbidities. This was considered justification for an in-person review.
The use of professional tools such as the BSSH and BAHT triage guidelines
10
and the Chartered Society of Physiotherapist (CSP) audio-visual service design toolkit
11
was reported by an additional 19% of the units. Staff confidence was reportedly increased by the use of guidelines from reputable clinical bodies. However, the absence of an individualised approach to mitigate clinical risk to patient outcome was noted. Whilst several units recognised the need for flexibility during the early stages of the response, the need for a valid and reliable tool to support decision making around the use of audio-visual services was acknowledged. ‘A lot of staff were initially re-deployed so F2F (face to face) appointments were very limited to patients having problems and post op. Since staff returning we are developing more robust criteria and will be using more audio-visual appointments for initial consultation’. Respondent 22
The decision to offer audio-visual consultations was made by a range of professionals but no consensus existed for how the decision was determined, justified or recorded. A method to objectively determine and justify the patient attendance in person was recognized as essential to support healthcare professionals in this new way of working.
Discussion
Although issues or concerns were raised by most services (92%) regarding the use of audio- visual consultation, the overall impression was positive. Examples of successful audio-visual use included: advice services, remote trauma clinic follow-up and the triage of minor injuries. Responses indicated that a season of unparalleled flexibility had led to technology-enabled care as a ‘valuable addition to our services’. As such, teams were keen to embrace the opportunity to develop new ways to support patients, with the caveat that the use of digital technology had limitations and ‘should not fully replace face to face contact’ for certain patients.
Taking a “lessons learned” approach, this study questioned the selection criteria for patients presenting with upper limb injury to determine the choice of either audio-visual or in-person consultation. This uncovered difficulties that were encountered when using audio-visual technology-enabled service versus the traditional in-person consultation. Hand therapy units from across the UK responded to the survey, with a broad range of location, size and demographics in the populations served. Identified themes revealed patterns in shared experiences, both positive and negative. The ability by specialist units to support peripheral services in the timely assessment and identification of cases that needed surgical intervention was also highlighted. Limitations in the management of upper limb injuries were apparent when treating complex injuries, differentially diagnosing closed trauma and managing exacerbations of chronic conditions.
The desire to retain and develop piloted services post COVID-19 is evident. However the complex nature of hand injuries in particular, revealed gaps both in safe audio-visual service provision and in the support of clinical staff to make decisions confidently. Findings from this study point to four strategic priorities required to ensure safe clinical practice and optimal patient care when choosing to use audio-visual technology in the management of upper limb injuries:
Firstly, a need to invest in access to audio-visual technology and equipment: Although previous studies have highlighted that subsets of patients could benefit from the use of audio-visual consultations,13,14 limited uptake prior to the pandemic was noted, with only 16% of services reporting pre-existing digital services. Whilst rapid service developments were expected to bring challenges, significant delays in the ability to offer audio-visual consultation were reported, with an average of 28 days taken to be operational. The main reason noted for this was an absence of investment to date in technology infrastructure and equipment. This included quality of Wi-Fi signal and remote access to investigations, such as radiographs, MRI and ultrasound scans. Staff reported unsustainable examples of team members working from home to access consistent signal, using personal equipment or sitting in hot-spots outside the clinical area to ensure strength of signal.
Whilst many units acknowledged that the COVID-19 response had created opportunities for staff to gain familiarity with available technology, it remained unclear how a lack of consistency between NHS Trusts, as to the platform and process used for remote consultation, would impact patient care. For digital transformation to be possible, investment in quality technology and equipment is required. Standardised protocols, policy and training that support clinical staff during this transition are integral to the provision of quality digital services.
Secondly, a need to ensure equitable access for patients to technology-enabled services: Benefits of technology-enabled services such as the promotion of self-management and an ability to support vulnerable patients and staff through the physical, psychological and social impact of the COVID-19 pandemic were expressed. The capacity to offer personalised care to those who were unable to attend in-person was highlighted. However, disparity in socio-economic status and confidence with technology were common concerns for respondents when offering remote consultation. An inability to purchase or access the technology required to use clinical services remotely created inequity between patients. Furthermore, communication barriers were noted for certain patients, including those with pre-existing disability, language barriers and mental health conditions. Any future clinical decision-making tools should be developed with input from patients representing these groups.
The findings of this study are in agreement with our experience at Salisbury Hospital Foundation Trust that remote consultation for the outpatient management of limb injuries has, to date, been under-utilized. Indeed, it could be effective for vulnerable groups such as prisoners, deployed UK personnel, those facing long journeys for review, and for continuity in care during inclement weather and disease outbreak. 13 Investigation into inclusive strategies to ensure equitable access for patients to the use of technology-enabled care should be prioritised by NHS leadership. Particular attention should be given to legal implications and consent.
Thirdly, the need for systems that identify and mitigate for clinical complications: Mitigation of clinical risk and optimization of clinical outcome commanded a significant focus for respondents. Prevention of complications, both post-operatively and in non-operative cases, was reliant on early identification of risks and timely access to review for each patient. Although many patients received advice and care remotely, the option to review in person when necessary was considered important. Primary reasons included an ability to assess wounds, palpate and, where indicated, manipulate tissues, as well as to create bespoke splinting to prevent deterioration.
Staff reported concerns with the accuracy and reliability of performing assessment remotely. Objective assessment, including goniometry, dynamometry and access to images were considered necessary for the success of clinical services. When these tools are not available remotely, findings suggested a lack of objective data had the potential to impact clinical reasoning and outcomes. Solutions proposed by survey respondents focused on the need for standardised assessment, both in terms of assessment tools and decision-making process. Particular recognition was given for the need to determine how the use of traditionally manual assessment methodology such as goniometry and dynamometry could be adapted for remote consultation. 15
Lastly, the need for a standardised decision-making process within and between units: The decision to offer audio-visual over in-person appointment consultations required the consideration of a number of factors. These included COVID-19 exclusion factors, the use of professional guidelines and clinical determinants. Additional service development algorithms such as the Chartered Society of Physiotherapists (CSP) toolkit 11 were reportedly used by 19% of units. Existing algorithms were felt to be of good quality, but gaps were identified at the point at which a clinical decision was to be made, justified and recorded. Whilst most respondents reported confidence in their unit’s ability to protect patients from COVID-19, no consensus existed for how to objectively measure and record the clinical indication for patient attendance in person. Survey results demonstrated that confidence in decision making centred on the use of clear guidelines and criteria, with 73% reporting the use of criteria to aid their reasoning. A need for a standardised and safe decision decision-making process within and between clinical units is critical to ensure parity and standards of care. This study suggests a need to develop valid and reliable tools to ensure the safe management of patients audio-visually.
Implications for future use of audio-visual technology
With continued vigilance called for in the face of a potential resurgence of COVID-19 and winter pressures, the role of audio-visual technology will be central to NHS service planning.1–3,5–7 Respondents recognised the current political will and investment as an opportunity to build a system for the management of upper limb trauma that incorporates the best of the Digital First agenda with the lessons learned during the response. Although this study uses upper limb injury as a lens to review decision making around audio-visual care, findings and the proposed need for standardised process and tools has implications for clinical services more broadly.
Study limitations
The study targeted hand service leads due to their position and knowledge and the timely need to collect data. As no single list of hand units existed, a combination of sampling methods was used to optimise recruitment, working from a best estimate of units offering upper limb trauma services in the UK (70–100). Where gaps existed, best efforts were made to identify and contact teams; however some potential participants may not have been detected. The study relied on self-report by respondents, which may not have fully represented the views or experience of the full team.
Conclusions
The choice of safely managed remote care or in-person consultation has, to date, largely relied on the discretion of the clinician. This survey reports a need for a carefully designed clinical decision-making tool for the management of upper limb trauma, both for use in clinical practice and future service planning. The use of evidence-based clinical criteria, alongside broader policy and service delivery guidelines, would ensure that care plans remain holistic and patient-centred, whilst building on the legacy of digital transformation.
This survey forms the first part of a series of work to explore the use of audio-visual technology in the management of upper limb trauma care and build the case for an evidenced-based, decision-making clinical tool. The results are timely in the current context where the pressures of robust winter planning, recovery of the service backlog and re-surge capacity management will be of concern for NHS capacity.
Supplemental Material
sj-pdf-1-hth-10.1177_1758998320972132 - Supplemental material for Clinical decision making in the provision of audiovisual care for upper limb trauma: a survey of UK experiences
Supplemental material, sj-pdf-1-hth-10.1177_1758998320972132 for Clinical decision making in the provision of audiovisual care for upper limb trauma: a survey of UK experiences by Emily McMullen, Megan Robson, Mark Paul Brewin, Poonam Valand, Leela Sayed and Jessica Steele in Hand Therapy
Footnotes
Acknowledgements
We would like to thank the British Association of Hand Therapy (BAHT) for distributing the survey and the members that responded. To Mr Henk Giele for his initial advice and expertise in the development of the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Salisbury NHS Foundation Trust research and ethics team were approached for advice and approval (12/06/2020). Due to the survey service evaluation format and no patient involvement, formal ethics approval was not required. However, the project was logged and a relationship maintained with the committee. A statement of intent was included in the survey introduction and an email indicated publication intent. Implied consent was therefore given by completion and submission of the survey. All researchers were GCP trained.
Guarantor
EJM.
Contributorship
EJM, MR, PV, LS and JS contributed to the study’s conception and design. The original concept was by EJM. EJM and MR designed and analysed the survey and EJM drafted the original version of the manuscript. MPB provided oversight and scientific knowledge in the revision of manuscript drafts. All authors revised the manuscript critically for important intellectual content and read and approved the final version. All authors agree to be accountable for all aspects of the work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.