
Abstract
Background
The radiation dose of coronary computed tomography (CT) angiography (CCTA) is generally higher than that of CT scans of other parts of the body, and there is concern that the high radiation dose may result in increased cancer risk. Although various techniques have recently been introduced to lower the radiation dose of CCTA, there has been no direct comparison between protocols with 80 and 120 kV.
Purpose
To assess the image quality and radiation dose of 80-kV electrocardiography (ECG)-gated CCTA in subjects with a normal body mass index (BMI), compared to 120-kV ECG-gated CCTA.
Material and Methods
This retrospective study was approved by our local ethics board, and the requirement of written informed consent was waived. We analyzed the CCTA images of 100 subjects with BMIs < 25 kg/m2. Fifty subjects underwent 120-kV CCTA, and the other 50 subjects underwent 80-kV CCTA. Two blinded observers independently evaluated the subjective image quality of the coronary arteries. The objective image quality (signal-to-noise ratio [SNR] and contrast-to-noise ratio [CNR]) and radiation dose were also measured in each group.
Results
Although the objective image quality of the 80-kV protocol images was significantly poorer than that of 120-kV protocol images (mean SNR, 14.9-4.7 vs. 19.8-4.4, P < 0.0001; mean CNR, 15.2±4.8 vs. 21.6-4.7, P < 0.0001), there was no significant difference in the subjective image quality between the two groups (mean image score, 4.7-1.1 vs. 4.5-0.7 for radiologist 1, P = 0.273; 5.0±1.0 vs. 4.8±1.0 for radiologist 2, P = 0.197). The radiation dose was reduced by 70% with the 80-kV protocol and by 88% with the 80-kV and ECG-based tube current modulation than with the 120-kV protocol (3.42±1.16 and 2.9±0.8 vs. 11.49-3.62 mSv, P < 0.0001).
Conclusion
The low tube voltage CCTA protocol using 80 kV allows significant reduction of the radiation dose without impairing the subjective image quality in subjects with normal BMIs.
Coronary computed tomography (CT) angiography (CCTA) is an accurate and non-invasive tool for excluding the possibility of obstructive coronary artery disease (CAD) in symptomatic subjects who have an intermediate pre-test probability of CAD (1–3). 64-slice CT scanners are widely used for CCTA, and the frequency and range of their applications have been extended. However, the radiation dose of CCTA is generally higher than that of CT scans of other parts of the body, and there is a concern that the high radiation dose may result in increased cancer risk (4,5). In particular, 64-slice CCTA with typical retrospective electrocardiography (ECG) reconstruction, the effective radiation dose is approximately 15–20 mSv on average when other techniques are not implemented to reduce the radiation dose (4). There have been considerable efforts to lower the radiation dose and prevent an overdose in subjects undergoing CCTA (6). New techniques have recently been introduced to lower the radiation dose such as ECG-based tube current modulation or prospective ECG gating technique.
Many investigators have already reported that lowering the tube voltage from 120 to 100 kV reduces the radiation dose without affecting the objective and subjective diagnostic quality of coronary artery images (7–10). Furthermore, a recent study observed that a tube voltage of 80 kV could also be applied for CCTA without impairing the image quality in slim subjects (11). However, they only applied the 80-kV protocol for patients with body weight < 60 kg irrespective of the height, and no other comparisons of their protocol with other tube voltage protocols were performed. Several studies have shown that a tube voltage of 80 kV can be used for pulmonary CT angiography and chest CT scans without impairing the diagnostic quality (12–14). However, there has been no direct comparison of protocols using 80-kV with the 120-kV protocol for CCTA, and no objective standard has been established for slim subjects.
The purpose of this study was to assess the feasibility of performing 80-kV ECG-gated CCTA in subjects with normal body mass indices (BMI) with that of 120-kV ECG-gated CCTA for obtaining good image quality and reducing the radiation dose.
Material and Methods
Study population
This retrospective study was approved by our local ethics board; the requirement for written informed consent was waived. We analyzed the data of the asymptomatic, self-referred, consecutive subjects who underwent CCTA during general medical examinations from January to June 2009 at our institution. From January to March, most of the subjects underwent CCTA using a 120-kV protocol. To reduce the radiation dose, we applied the ECG-based tube current modulation technique for subjects whose heart rate was below 65 beats per minute (bpm). In our institute, ECG-gated cardiac CT has been performed in subjects with atrial fibrillation before they undergo radiofrequency catheter ablation. The tube voltage of the CT scanner was preset at 80, 120, and 140 kV, and we utilized the lowest dose of 80 kV in the CT protocol because the primary purpose of cardiac CT was to evaluate the left atrium and pulmonary vein and not to evaluate the coronary arteries. We ensured that the coronary artery in subjects with normal sinus rhythm and BMI < 25 kg/m2 could be evaluated. Therefore, we performed low tube voltage CCTA using 80 kV in consecutive subjects with BMI values < 25 kg/m2 in the latter half of the study period. Patients with arrhythmia were excluded before the scan. Subjects were also excluded when the CCTA image quality was poor for the evaluation of coronary artery stenosis due to respiratory motion artifacts. Finally, 50 subjects who underwent CCTA using the 120-kV protocol and another 50 subjects who underwent CCTA using the 80-kV protocol were enrolled.
CCTA protocol
The ECG-gated CCTA studies were performed using a 64-detector-row CT scanner (Brilliance 64; Philips Medical Systems, Cleveland, OH, USA). Standard coronary imaging protocols were applied, including the use of an oral beta-blocker (metoprolol: Betaloc; AstraZeneca, Seoul, Korea) for subjects with heart rates > 65 bpm (unless contraindicated), and 0.6 mg of sublingual nitroglycerin (Myung Moon Pharm, Hwasung, Korea) was administered to all of the subjects. An 80-mL bolus of contrast agent (iopromide: Ultravist, 370 mg I/mL; Bayer Schering Pharma, Berlin, Germany) was injected intravenously at a rate of 5 mL/s, and a 40 mL mixture of saline and contrast agent was subsequently injected as a chaser (a ratio of 7:3). When the density in the ascending aorta reached a predefined threshold of 100 Hounsfield units (HU), the scan started automatically with a 6-s scan delay, and the entire volume of the heart was scanned during one breath-hold of 8-10 s with simultaneous recording of the ECG trace. The imaging parameters were as follows: slice collimation, 64 × 0.625 mm2; gantry rotation time, 420 ms; tube voltage, 120 kV; tube current, 800 mAs. Low tube voltage CCTA was performed using a tube voltage of 80 kV instead of 120 kV and a tube current of 1000 mAs with the same slice collimation and rotation time.
The ECG-based tube current modulation technique for reducing the radiation dose was used for subjects with mean heart rate < 65 bpm; the full tube current was applied from 60% to 80% of the R-R interval. The ECG-based tube current modulation technique was used in 36 subjects of the 120-kV protocol group and 38 subjects of the 80-kV protocol group. Using retrospective ECG gating, the optimal phase that provided the best image quality was chosen. The axial CT images were reconstructed with a slice thickness of 0.8 mm, an increment of 0.5 mm, and the use of a sharp reconstruction filter (Xres Sharp).
Image analysis
The CT data analysis was performed by two radiologists who had 8 and 2 years of experience in cardiovascular radiology, respectively. The images were reviewed and analyzed on a G3 PACS system (Infinitt Co., Ltd., Seoul, Korea). To objectively evaluate image quality, the attenuation (in HU) of the four territories (the left main coronary artery [LM], right coronary artery [RCA], and perivascular tissue of each of the arteries) and the standard deviation of the descending thoracic aorta attenuation (in HU) were measured in transverse views (7). The attenuations were measured in a region of interest (ROI) in the proximal segment of the RCA and LM, and these ROIs were defined to be as large as possible while avoiding calcifications, plaques, and stenosis (Figure 1). The image noise was determined as the standard deviation (SD) of the attenuation value of the ROI placed on the descending thoracic aorta. The signal-to-noise ratio (SNR) and the contrast-to-noise ratio (CNR) were calculated by the following formulae (7):

(a, b) Transverse images (120-kV protocol) of a 54-year-old man with BMI of 24.6. (c, d) Transverse images (80-kV protocol) of a 50-year-old man with BMI of 24.1. Attenuations were measured in the proximal segment (black dot) and perivascular area (white dot) of the right coronary artery (RCA) and left main coronary artery (LM), and the region of interests (ROI) were defined to be as large as possible, while avoiding plaques, calcifications, and stenosis. The image noise was determined as the standard deviation of the attenuation value in the ROI that was placed in the descending aorta (dashed circle)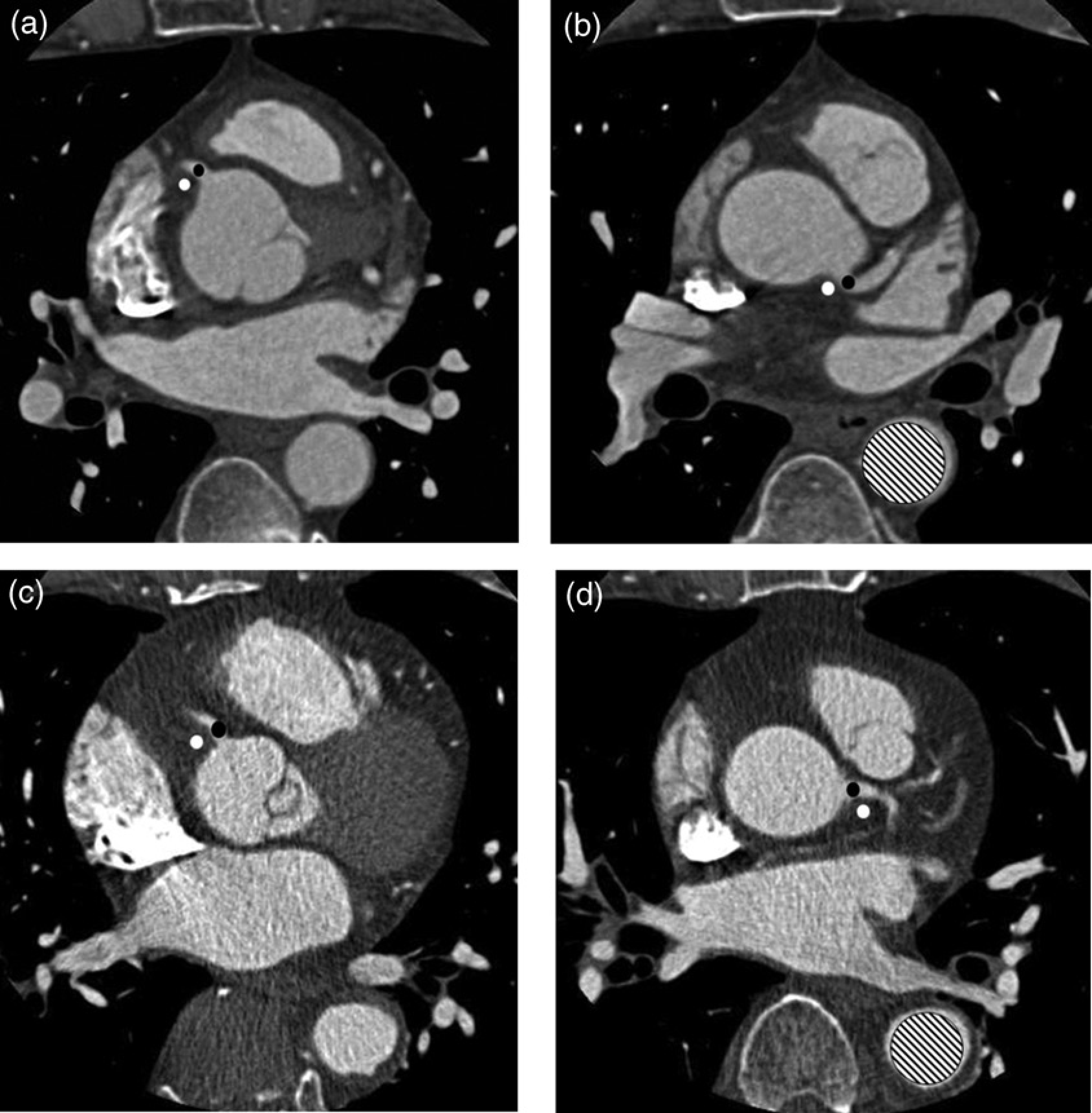
The images from the two protocols (80-kV and 120-kV protocols) were analyzed by two radiologists. To subjectively review the images, they independently performed a “blinded” and randomized qualitative image analysis of the RCA, LM, left anterior descending artery (LAD), and left circumflex artery (LCX). The image quality of each coronary artery was evaluated on a 4-point scale using axial and multiplanar reconstructed CT images as follows: 1, excellent image quality without any artifact throughout the coronary artery; 2, acceptable image quality, not compromising the assessment of the vessel; 3, non-diagnostic image quality for a single segment within the coronary artery; and 4, non-diagnostic image quality for multiple segments within the coronary artery (10). Fifteen segment-based analysis of the subjective image quality of the coronary artery was also performed by the radiologist, who had 8 years of experience in cardiovascular radiology. The image quality of each coronary segment was scored as follows: 1, excellent image quality without any artifacts; 2, acceptable image quality, not compromising assessment; and 3, non-diagnostic image quality. Each segmental score was added, and the mean value was calculated.
The curved planar reformatted images of the coronary artery and the volume-rendered images of the different tube voltage CCTA protocols were also reconstructed but not used for qualitative image analysis.
Estimation of the CT radiation dose
The CT radiation dose was compared between the two groups. The volume computed tomography dose index (CTDIvol) and dose length product (DLP) of each protocol were reported. The effective dose (ED) of each protocol was calculated according to the International Commission on Radiological Protection (ICRP) Publication 103 recommendations; the conversion factors for 120 and 80 kV were 0.0147 and 0.0145 mSv/mGy cm, respectively (15).
Statistical analysis
The continuous variables are expressed as means ± standard deviations (SDs), and the categorical variables are expressed as frequencies and percentages. The categorical characteristics were compared using the chi-square test, and the Student unpaired t test was used to compare the continuous variables. The interclass correlation test was used to assess the inter-observer reproducibility of the subjective image quality between the two readers. A Cronbach's α> 0.70 indicated a strong correlation, a value between 0.40 and 0.70 indicated a moderate association, and a value < 0.40 indicated a weak correlation. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) for Windows, version 12.0.1 (SPSS Inc., Chicago, IL, USA). Associations were considered significant at P values < 0.05.
Results
Baseline characteristics
There were no significant differences in age (49.9±11.2 [31–75] vs. 52.2±10.6 [32–72], P = 0.294), percentage of men (72% vs. 68%, P = 0.828), BMI (22.4±1.9 [16.9–24.7] vs. 22.6±1.8 [17.9–25], P = 0.626), and heart rate (56.6 ± 6.6 [44–71] vs. 56.5±7.0 [45–69], P = 0.988) between the 80-kV and 120-kV protocol groups. Six subjects in each group had BMIs < 20.
Objective and subjective image quality of the coronary arteries
The image noise, attenuation of the proximal RCA and LM, and attenuation of the perivascular area of the proximal RCA and LM were different according to the tube voltage of the CCTA. The mean image noise value of the 80-kV protocol was 2.5-fold higher than that of the 120-kV protocol (67.0±16.3 HU vs. 26.8±5.0 HU, respectively). The mean attenuation of the contrast medium in the RCA and LM was approximately 1.82-fold higher in the 80-kV protocol than in the 120-kV protocol. The SNR and CNR were higher for the 120-kV protocol than for the 80-kV protocol (Table 1).
The signal-to-noise ratio and contrast-to-noise ratio of the two groups of subjects imaged using low tube voltage and standard coronary computed tomography angiography protocols

CNR, contrast-to-noise ratio; LM, left main coronary artery; RCA, right coronary artery; SNR, signal-to-noise ratio
P, 0.05
The subjective image quality according to the different tube voltages of the CCTA protocols, the score of each vessel, and the sum of the four vessels’ scores by the two radiologists was not significantly different between the protocols (Table 2). The inter-observer reproducibility was excellent for the LAD (Cronbach's α = 0.713), and it was moderate for the other coronary arteries (Cronbach's a: 0.449 for LM, 0.502 for LCX, and 0.662 for RCA). The mean subjective image quality score of the 15 segments according to the different tube voltages of the CCTA protocols was calculated by one radiologist, and no significant difference was observed between the two protocols (1.1 ± 0.1 vs. 1.1±0.1; P = 0.96). The number of non-diagnostic segments (score of 3) was four for the 80-kV protocol and three for the 120-kV protocol. It resulted from motion artifacts due to heartbeats and mostly occurred at the mid-segment of the right coronary artery. The images were noisy when the tube voltage was decreased, whereas the image quality of the coronary segments remained diagnostic (Figure 2).
The subjective image quality scores by the two radiologists when using low tube voltage and standard coronary computed tomography angiography protocols

LAD, left anterior descending artery; LCX, left circumflex artery; LM, left main coronary artery; RCA, right coronary artery
The curved planar reconstruction images of the coronary artery and the volume-rendered images showing the image quality of the different tube voltage CCTA protocols (a–d, 120 kV; e–h, 80 kV). The images were partially noisy when the tube voltage was decreased, whereas the image quality of the coronary segments remained diagnostic
The objective image quality and the subjective image quality, according to the use of ECG-based tube current modulation, are summarized in Table 3. The subjective image quality as scored by radiologist 2 (who had 2 years of experience) was significantly better in the subjects who underwent ECG-based tube current modulation in the 80-kV protocol.
The objective and subjective image quality according to the use of electrocardiography-based tube current modulation

CNR, contrast-to-noise ratio; SIQ1, sum of the subjective image quality scores by radiologist 1; SIQ2, sum of the subjective image quality scores by radiologist 2; SNR, signal-to-noise ratio; TCM, electrocardiography (ECG)-based tube current modulation
Radiation dose estimates in relation to the applied CCTA protocol
The radiation dose parameters under the different CCTA protocols and ECG-based tube current modulation are summarized in Table 4. The differences in scan ranges between the groups did not reach statistical significance. The use of a reduced tube voltage of 80 kV resulted in significant reductions in the CTDIvol, DLP, and ED. Compared to the estimates of the 120-kV protocol, reducing the tube voltage resulted in overall DLP and ED reductions of 70%. The mean value of the estimated dose saved by tube current modulation was not significantly different between the 80-kV and 120-kV groups (22.48±14.97% vs. 27.60± 18.02%; P = 0.125). The additional reduction of the radiation dose by using the ECG-based tube current modulation was approximately 40%.
Estimation of the radiation dose in the groups of subjects who were studied using 80-kV and 120-kV protocols with electrocardiography-based tube current modulation

BMI, body mass index; CTDIvol, volume computed tomography dose index; DLP, dose length product; HR; heart rate; TCM, electrocardiography (ECG)-based tube current modulation
Discussion
In the present study, radiation exposure was reduced by 70% when CCTA was performed using the 80-kV protocol rather than the 120-kV protocol in subjects with normal BMI. There was no significant difference in the subjective image quality between the groups, although the objective image quality of the 80-kV protocol was poorer than that of the 120-kV protocol.
The increased utilization of CCTA has resulted in increased radiation exposure in the population. The median DLP of 1965 CCTA examinations performed at 50 study sites was 885 mGy cm (range of the median DLPs per site: 331–2146 mGy cm) (16). Several studies have attempted to reduce the radiation dose of CCTA. Leschka et al. (7) reported that dual-source CCTA with a tube voltage of 100 kV does not deteriorate the subjective quality of coronary arteries images, but rather increases the attenuation and the CNR and reduces the radiation dose from 8.9 mSv to 4.4 mSv in subjects with a normal body weight (18.5 < BMI < 25). Stolzmann et al. (8) performed CCTA with dual-source CT using a 100-kV protocol in subjects with a BMI < 25 kg/m2 and a 120-kV protocol in subjects with a BMI of 25–30 kg/m2. They found that there were no significant differences in the image quality between the 100-kV and 120-kV protocols, and diagnostic image quality was achieved with all protocols in 97.9% of the coronary segments. Hausleiter et al. (9) evaluated the image quality and radiation dose of the 100-kV tube voltage scan protocol. They randomly assigned 400 non-obese subjects to the 100-kV and 120-kV protocols, and concluded that a CCTA protocol using a 100-kV tube voltage maintained image quality, but reduced the radiation exposure by 31% compared with that of the 120-kV protocol. Pflederer et al. (10,17) also revealed that the low-dose CCTA protocol using 100 kV leads to a significant reduction in radiation exposure, and does not negatively influence the image quality in subjects with body weight <85 or 90 kg. In the recent guidelines for performing CCTA, reducing the voltage from 120 to 100 kV is recommended when the patient's weight is, 85 kg or when the BMI is, 30 kg/m2 (18). Some studies revealed that a tube voltage of 80 kV can be used in pulmonary CT angiography and for chest CT while maintaining diagnostic quality (12–14). Another study investigated whether a tube voltage of 80 kV could be used in CCTA while maintaining the diagnostic quality of the images (11). In that study, 11 slim subjects (body weight <60 kg) who required CCTA were evaluated using an 80-kV protocol. The overall image quality was subjectively rated on a 5-point scale, and was good in all cases. The mean SNR value was 10.9±2, and the mean DLP value 122.5±28.6, which correspond to a radiation exposure of 2 mSv. They concluded that the dose of radiation exposure can be reduced by up to 88% for slim subjects without impairing the image quality. However, there has been no direct comparison of the 80-kV protocol with the 120-kV protocol, and the aforementioned studies only assessed the image quality by subjective consensus analysis.
Our current study showed that lowering of the tube voltage from 120 to 80 kV in the subjects with a BMI <25 kg/m2 allows the subjective image quality to be maintained. Despite the difference in experience between these two radiologists, the subjective image quality scores between the observers were very similar, as the interclass correlation test indicated moderate to excellent inter-observer reproducibility. Furthermore, the subjective image quality of each coronary segment, which was analyzed by one radiologist, was also similar between the two CCTA protocols.
For the low tube voltage protocol using 80 kV, the image noise was increased by a greater proportion than the increase in the attenuation of the contrast medium, and this resulted in a decrease in the objective image quality, as expressed by the CNR and SNR. However, to the best of our knowledge, there is no consensus about the optimal values of the CNR or SNR for acceptable objective quality. Leschka et al. (7) indicated that the CNRs were significantly higher for 100 kV/330 mAs and 100 kV/220 mAs protocols than for the 120-kV protocol (25.5±3.2 and 25.0±2.2 vs. 20.6 ±1.7). In the PROTECTION II Trial, the objective image quality in the subjects scanned using the 100-kV and 120-kV protocols was not different (CNR, 13.6±6.0 vs. 14.8±6.4) (9). A previous study of pulmonary CTA using either 80-kV or 120-kV protocol showed that the CNR for the pulmonary trunk did not differ between the groups (7.10 vs. 7.82) (13). Leber et al. (19) previously defined the CNR for assessable vessels as > 3. Karaca et al. (20) defined CNR levels as follows: >8, high quality image; 4–8, moderate quality image; and <4, poor quality image. Accordingly, although our results for the CNR and SNR of the 80-kV protocol are lower than that in previous low tube voltage CCTA studies using 100 kV, they are acceptable for practical examinations.
Our strategy to reduce the radiation dose during CCTA was to both apply the ECG-based tube current modulation technique and lower the tube voltage. The study showed that lowering the tube voltage from 120 to 80 kV in subjects with a BMI < 25 kg/m2 reduces the radiation dose by up to 70%. Compared with that of the 120-kV protocol without using ECG-based tube current modulation, the low tube voltage protocol using both 80kV and ECG-based tube current modulation reduced the radiation dose by 88%. Of course, when iterative reconstruction is used in CT, the radiation dose is reduced by 32–65%. Additionally, advanced CT scanners also reduce the radiation dose while maintaining a high image quality (21). However, the present study was performed with a 64-slice multidetector CT, which is currently the most commonly used CT scanner.
There were some limitations of this study. First, the sample size was relatively small. Subgroup analysis was impossible because the number of subjects with BMI <20 was only six for each group. Second, presence of stenosis or plaque on CCTA images was not evaluated, therefore further evaluation is needed. Finally, the population consisted of asymptomatic self-referred subjects who underwent a general medical examination, and the diagnostic accuracy of 80-kV CCTA was not evaluated. We admit that low kV technique may hamper the diagnostic accuracy of CCTA when heavy coronary artery calcium is present.
In conclusion, the low tube voltage CCTA protocol using 80 kV showed no significant difference in subjective image quality and was equivalent to that of the 120-kV protocol in subjects with a BMI <25 kg/m2. The 80-kV protocol significantly reduced the subjects’ radiation dose by 70%. Therefore, the 80-kV protocol CCTA can be applied to subjects with normal BMI, and BMI should be considered before performing CCTA.