
Abstract
Leg telangiectasias resistant to repeated courses of sclerotherapy in patients without deep and superficial venous incompetence are not uncommon. Little is known about factors which may underlie the resistance. Among 26 patients with such telangiectasias we found a direct communication of the vessels with deep and saphenous veins in 65% of patients. Ultrasound-guided injection of 0.5% polidocanol foam into the feeding veins or their perforating segments led to clearance of all the telanagiectasias. In 23% of cases no feeding veins could have been identified by ultrasound. Direct injections of a sclerosant into perforating feeding veins may clear refractory telangiectasias in a majority of patients though it is obvious that other factors may contribute to the failure of sclerotherapy in others.
Introduction
We and others presented evidence that some lower extremity telangiectasias (9–13%) are directly connected to deep veins via a perforating vessel, irrespective of the competence status of the saphenous and deep veins.1, 2 Clinical consequences of the connection were mainly limited to, but never formally proved, explanation of some rare cases of deep venous thrombosis after sclerotherapy of leg telangiectasias. Every phlebologist performing sclerotherapy of leg telangiectasias has encountered patients with some of the vessels not responding to standard treatment. However, possible underlying mechanisms of the resistance have never been systematically explored.
We have noted that in many cases of treatment-refractory telangiectasias, one can trace by ultrasonography a perforating vein connecting the feeding subcutaneous vein beneath the telangiectasias with a deep vein, mostly in the leg. Unless the perforator is sclerosed, the visible cutaneous vessels will not usually disappear.
Case series
We have seen 26 patients with treatment refractory lower extremity telangiectasias over a 12-month period. Only one patient had been on an oestrogen replacement therapy. All of them had previously undergone at least three sessions of compression sclerotherapy with 0.5% polidocanol foam into telangiectasias and feeding reticular veins if they had been found. At least at one site the treatments were unsuccessful at eradicating the vessels. All of the patients underwent duplex ultrasound investigation and did not have incompetence within either the superficial or deep venous systems. In an attempt to find a reason for treatment failure, we performed a careful inspection and ultrasound examination of the area beneath the refractory telangiectasias. Treatment refractory telangiectasias were mostly found on lower legs – in only three patients they were located on the thigh. Though a higher number of the vessels were found on the posterolat-eral aspect of lower legs, the difference as to the site was not statistically significant. A feeding reticular vein has been rarely seen to connect to the telangiectatic flares (Figure 1). Yet by ultrasound we identified several different situations (Figure 2): in 14 patients (53.8%) a subcutaneous feeding vein running from beneath the telangiectasia connects to a deep vein via a perforator vessel; in six patients (23%) there has not been any US-detectable connection between the telangiectasias and the feeding or perforating vessels; in three patients (11.5%) a feeding subcutaneous vein was seen, but apparently not connected to a deep or spahenous systems; in three patients (11.5%) a feeding subcutaneous vein drained into the small saphenous vein (2 patients) or anterior accessory great saphenous vein (1 patient). The diameter of the feeding or perforating vessels ranged from 1.5–3.5 mm (Figure 3). There were no specific clinical patterns of telangiectasias connected to perforators – any of arborized, spider, linear, papular and their combination may be found (Figure 1).
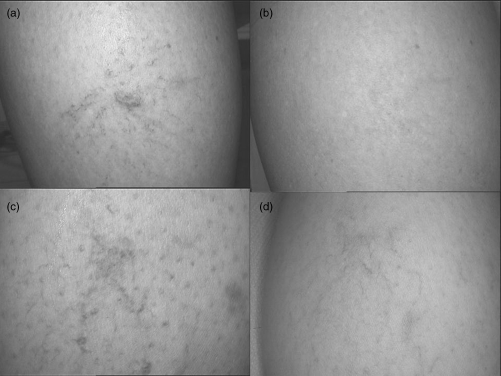
Sclerotherapy-refractory telangiectases on the lower legs (a, c) before and 16 (b) and eight (d) weeks after sclerotherapy by 0.5% polidocanol foam injected into a feeding subcutaneous vein/perforator under the ultrasound guidance

Connection of refractory telangiectasias to other components of the venous system as identified by ultrasound scanning. SQV, subcutaneous vein
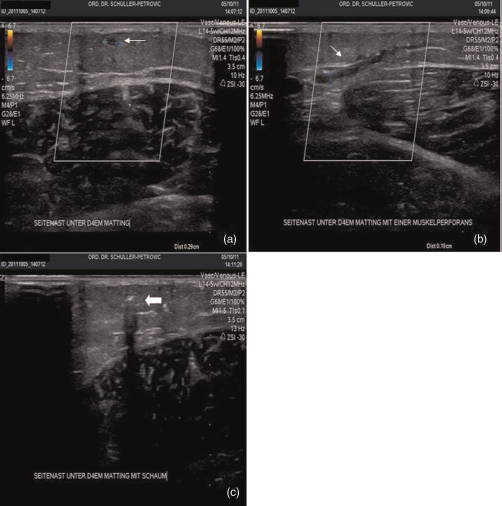
Ultrasound findings in a patient with sclerotherapy-refractory telangiectasias. Subcutaneous feeding vein beneath the telangiectasias (a) runs deep and pierces the muscular fascia (b). Foam injected into the feeding vein (c)
In order to close the telangiectasias we injected 0.2–0.5 mL of 0.5% polidocanol foam (according to Tessari; mixed with an air to polidocanol ratio 4:1) directly into the subcutaneous feeding vein or the perforator under the ultrasound guidance until the telangiectasias filled with the sclerosant foam (Figure 3c). Depending on the depth of the target vessel we used either 27- or 30-gauge needles. All of the patients retreated in this way had their telangiectasias completely or at least 75% cleared after three months (Figure 1). There have not been recurrences during the follow-up period ranging from 6 to 14 months. We have not encountered a single case of deep vein thrombosis.
Discussion
The issue of relationship between telangiectasias and feeding reticular veins regarding efficacy of sclerotherapy is still debatable.3, 4 It is however clear that some telangiectasias communicate with the deep and saphenous vein systems.1, 2 In this series of patients with resistant telangiectasias almost 65% of the vessels communicated with the deep or saphenous venous systems (Figure 2). When injecting telangiectasias with polidocanol foam not infrequently we follow foam signals in nearby saphenous veins or even deep veins (Schuller-Petrović and Pavlović MD, unpublished observations). We agree with observations of Green 3 and comments by Duffy 4 that reticular feeding veins are not crucial for eradicating telangiectasias (our own, unpublished, observations confirmed that in some cases it is better to avoid reticular veins treatment since there may be even higher incidence of telangiectatic matting) yet underscore that direct communication of some telangiectasias with deep veins via perforators, possibly due to higher intraluminal pressures, may make the vessels treatment resistant. Sclerotherapy resistant telangiectasias were found mostly on lower legs where perforators are otherwise more numerous, and where the length of the connection path is shorter. It should be noted that neither patient had detectable deep or saphenous vein incompetence. It is obvious that treatment success of sclerotherapy of telangiectasias without clear venous incompetence depends on many factors, the connection to deep venous system being probably one of them. Other still unknown variables must also be important as 34.5% of the sclerotherapy resistant vessels in this series did not show by ultrasound any direct communication with the deep or saphenous veins and two-thirds of them did not even have an apparent feeding vein. It is possible that the feeding vein in these cases is very small to be detected by standard ultrasound scanning. One must differentiate between resistance of telangiectasias to sclerotherapy and telangiectatic matting, the latter being the appearance of truly new vessels, probably as a result of impaired apoptosis of endothelial cells and neoangiogenesis. 5 It occurs mostly irrespective of the sclerotherapy technique or connection of telangiectasias to the deep venous system. However, impaired apoptosis might underly both phenomena. Though it is not practical to search for small perforators by ultrasound in any case of telangiectasias, it may be helpful to be aware of their importance in cases of refractory lesions.