
Abstract
BACKGROUND:
The most common cause of coronary artery disease (CAD) is vascular damage with the cholesterol built-up and other materials on the inner arterial wall, known as atherosclerosis.
OBJECTIVE:
This paper aims to investigate the effect of stenosis on the hemodynamics in the four suspected coronary artery disease patients. Computer tomography (CT) data was acquired from patients of suspected coronary artery disease to reconstruct left coronary artery.
METHODS:
The 3D computational simulation was carried out with four patient-specific models with area stenosis >50% located at the left anterior descending (LAD) and left circumflex (LCX) branches.
RESULTS:
The pressure, velocity and wall shear stress were calculated during the cardiac cycle. A significant pressure drop across the stenosis and increase in the velocity at the stenosis were observed at LAD and LCX branches. An increase in the wall shear stress in the region of stenosis also observed with the prevalence of the recirculation zone at the post stenosis region which results in the formation of stenosis.
CONCLUSIONS:
Our analysis provides an insight into the progression of stenosis and wall rupture, thus improving our understanding the flow behavior patient-specific realistic artery models.
Introduction
The human heart is one of the most important body organs whose wellbeing is critical for the functioning of the whole body. However, the heart itself requires sufficient blood supply to keep it in a healthy condition. The oxygenated blood to heart muscles are supplied by specific arteries termed coronary arteries. Thickening of the coronary artery wall which leads to narrowing of blood passage area is a common disease known as atherosclerosis. Atherosclerosis is known to have caused millions of deaths across the globe for many years and even today is one of the leading fatal diseases. The development of stenosis on the inner wall of artery results in reduced blood flow. There are various causes of stenosis formation primarily linked to food habits. There has been continuously growing interest to understand the blood flow behavior in the atherosclerosis condition due to its serious impact on human life. It is observed that the stenosis frequently occurs at the bifurcation or branching of vessels and curvature regions where a low wall shear stress is found [1,9,34]. It is also reported from previous studies that area stenosis (AS) >50% causes a significantly reduced volumetric blood flow rate [12]. The left coronary artery has more complicated geometry than the right coronary artery due to bifurcating with varying angles in different individuals [2,8,10]. Several studies described the coronary artery blood dynamics referred as hemodynamics and the formation of the stenosis by using computational fluid dynamics [7,11,17,23,26,30]. The wall shear stress and blood flow changes cannot be measured directly in coronary arteries [29]. The anatomical details of artery and any unwanted deposition that ultimately leads to formation of stenosis, are available through the advanced medical imaging techniques such as Computed Tomography Angiography and Angiography, but limited to the analysis of the flow variation in the coronary arteries [3]. Thus computational fluid dynamics provides additional information on hemodynamic variations with the help of the modern medical imaging techniques. The present study investigates the effect of stenosis present at the bifurcation of left coronary artery on the hemodynamic factors and wall shear stress based on the patient-specific reconstructed artery models. These results can be used to analyze the development of stenosis in the coronary arteries.
Methodology
The CT scan data of four patients suspected to have coronary artery disease were obtained. CT Angiography was performed on 128 slicer scanner for all the four patients with the following specifications: the beam collimation 0.6, pitch 1.4, reconstruction interval of 0.6 mm with the tube voltage of 100 kVp current ranging from 300 to 650 mAs. Axial images were reconstructed with a slice thickness of 0.6 mm in 0.75 mm increment. The demographics of patients used in the current study is shown in Table 1. The approximate morphology of the stenosis present in the left coronary arteries segmented by using CT scan images is shown in Fig. 1.
Patient’s details of suspect’s coronary artery disease
Patient’s details of suspect’s coronary artery disease
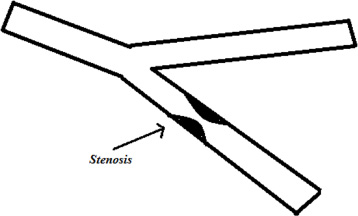
The schematic diagram of approximate morphology of the stenosis.
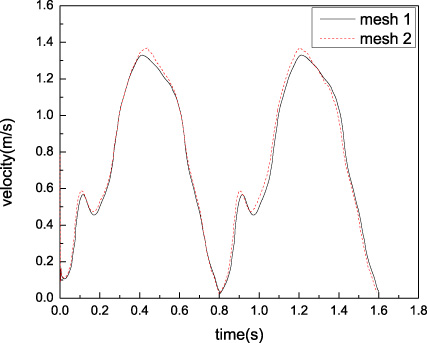
The DICOM images obtained from all the four patient were imported to commercially available software MIMICS-18 (Materialise, Leuven, Belgium). By using the thresholding function and creating a 3D mask, an optimized model of left coronary artery with side branches was segmented as shown in Fig. 2. The surface models of left coronary artery were saved in Stereolithography (STL) file format. The 3D surface models of left coronary artery were imported into meshing software 3-matic in order to further smoothen and create a fine tetrahedral mesh consisting of 167309 tetrahedral elements. A mesh independent study was carried out before selecting above said number of elements. Figure 3, along with Table 2, shows the details of mesh independent study.
Mesh independent study for model D
Mesh independent study for model D
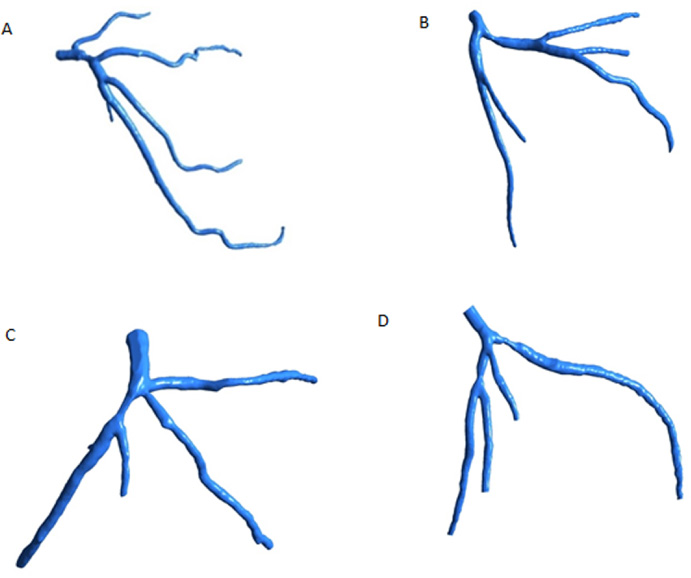
The reconstructed left coronary artery models with stenosis. Each model corresponds to individual patients.
Comparison of mesh independent study for different number of elements.
Blood is assumed to be non-Newtonian, incompressible and governed by the Navier-Stokes equations.
The governing equation for the non-Newtonian and Bird-Carreau model given by
It is well known fact that the activation of endothelial cell by the shear stress and localisation of plaque are closely related. The wall shear stress is calculated based on the following equation.
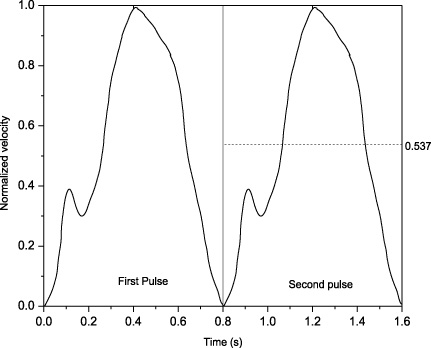
A realistic in vivo model was reconstructed by applying the transient pulsatile velocity at the inlet as shown in Fig. 4. A static pressure boundary conditions of 80 mmHg at the outlet, with no-slip boundary condition was applied at the wall, since the rigid wall is assumed [28]. All the four real LCA models were solved with the same boundary conditions in the present numerical scheme. The modeling was accomplished with shear stress transport (SST) model, a k-𝜔 model generally used for high Reynolds number flow.
Figures 5, 6, and 7 depict the variations in the hemodynamic parameters such as pressure, velocity and wall shear stress respectively under the hyperemic conditions for the time step 1.2 seconds. The results of the present study provide necessary information of the significant influence of the stenosis on the hemodynamic parameters through which the subsequent effect on blood flow characteristics can be inferred for hyperemic conditions.
Figure 5 illustrates the pressure variation in the left coronary artery of all four patients due to the stenosed area in the artery. It is evident from Fig. 5 that the pressure of the blood flow decreases in the post stenosed area, which is common phenomenon due to obstruction presented by presence of stenosis in the blood flow pathway. The stenotic resistance increases the pressure due to blockage effect in the area before stenosis whereas the pressure drops due to expansion after the stenosis. The pressure drop is one of the important parameters in assessing the severity of stenosis. The fractional flow reserve (FFR) which is used as judgment tool to assess the severity of blockage is based on pressure drop across the stenotic region [13,15,24,27]. The higher the pressure drop, the more severe the condition of the patient is. The variation of pressure depends on the blood flow rate dictated by various physiological conditions. The pressure drop across the stenosis at LAD branch is found to be in the range of 14300 Pa to 13670 Pa as shown in Fig. 5A. The pressure drop in Fig. 5B is in the range from 11490 Pa to 11230 Pa across the stenosis at LCX branch. Similarly, the pressure drop is found to be in the range of 10540 Pa to 10300 Pa and 11000 Pa to 10780 Pa respectively for the stenosis located at LAD as seen in Fig. 5C and 5D respectively.
Likewise, Fig. 6 demonstrates the change in velocity due to the stenosed area in the artery during the hyperemic conditions for 1.2 s time step. The velocity increases at sharp rate at the stenosis region. This happens because of conversion of pressure energy into kinetic energy due to pressure drop. The velocity is found to be affected beyond the stenosis region due to the reduction in the arterial area. The blood velocity increased from 0.95 m/s to 1.67 m/s at the LAD (Fig. 6A), whereas the increment of 0.8 m/s to 1.6 m/s could be seen at the LCX as shown in Fig. 6B (model 6B). In the same way the velocity increased from 0.94 m/s to 1.69 m/s at LCX Fig. 6C (model 6C) and from 0.78 m/s to 1.4 m/s at LAD (Fig. 6D). The increment of velocity is consistent with other studies being carried out for normal flow conditions [14].
Similarly, the effect of stenosis on the wall shear stress is depicted in Fig. 7. The wall shear stress has significance due to its role in determining the artery strength. The higher wall shear stress may lead bursting or rupturing the arterial wall. It is well known that the high wall stress may create raptures and low wall stress helps in fatty or other undesirable substances to get deposited on arterial walls thus further increasing the stenosis region [16,18,31,33]. It is also reported that the normal LAD has a wall shear stress value of 12 Pa [32]. It is noted that the wall shear stress is also significantly increased across the stenosis at LAD and LCX branches. The maximum significant wall shear stress for four patients is found to be 91 Pa, 50 Pa, 65 Pa and 51 Pa respectively as illustrated in Fig. 7A, 7B, 7C and 7D respectively.
Discussion
This study presents the variation of flow changes and wall shear stress distributions in the left coronary arteries based on the patient-specific CT angiograms. The finding of this study could be useful in predicting the progression of atherosclerosis in the coronary arteries. The previous studies reported that stenosis frequently occurred near the bifurcation, due to the angulation between LAD and LCX and tortuosity which could lead to low wall shear region at bifurcation [2,9]. It is well proven through clinical and experimental studies that the wall shear stress and pressure play which are termed as biomechanical forces have vital role in deciding the development of coronary atherosclerosis. The variation in the wall shear stress affects the function of endothelial cell. Longitudinal animal and human studies have shown that coronary regions with low WSS undergo increased plaque growth compared with high WSS regions. In the current study, highest wall shear stress to be observed was that of 91 Pa at LAD model (Fig. 6A). This is very high value compare to the normal condition at the stenotic locations and this seems to indicate that the stenosis may rupture at high wall shear stress locations. Furthermore, a recirculation area immediate to the stenosis was noticed which leads to low wall shear stress. The recirculation area is created due to low pressure zone thus having very low velocity blood flow pertinent to that particular area. The absence of sufficient blood flow hinders the cleaning of adhesives such as fat or calcification etc. in that particular region. Thus, it renders the recirculation region into a safe place for deposition of undesirable material. According to the analysis it is found that low velocity region at post stenosis could lead to the formation of new stenosis. These results obtained in the current study are consistence with the previously published data [3–5,19–21]. It is known that disturbed blood flow leads to highly heterogeneous, and often contradictory, behavior of Endothelial cells at atheroprone sites [6,25]. The activation of c-Jun N-terminal kinase 1 is caused by disturbed flow that induces endothelial cell apoptosis.
The present study of hemodynamics analysis of patients with realistic left coronary has some limitations, the wall of left coronary models were assumed as rigid, this assumption is reasonable in this case [17]. The size of the stenosis in all 4 patients is >50% but the exact size could not be determined due to limitations of available data.

Visualization of pressure distribution of four patients in the left coronary artery for time step 1.2 s.
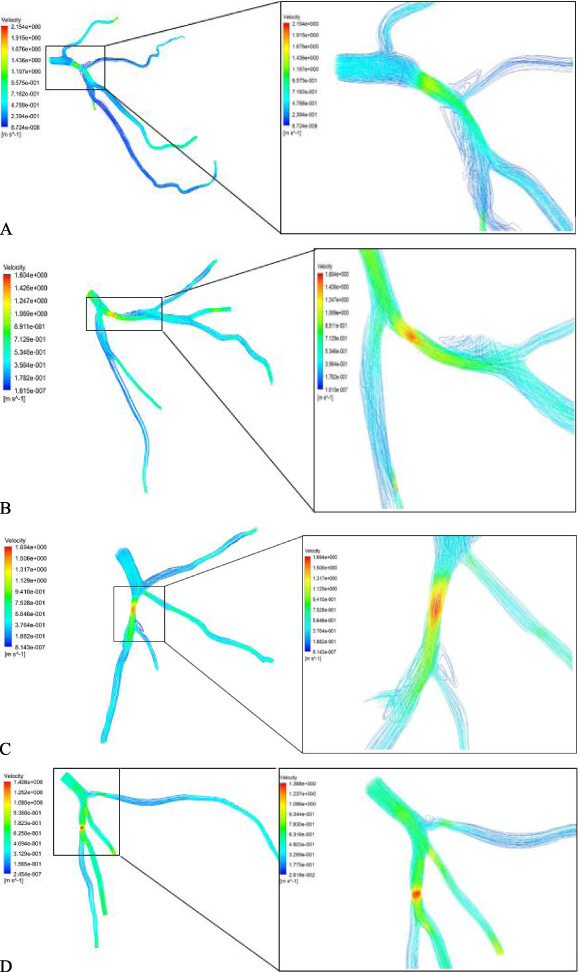
Visualization of velocity pattern of four patients in the left coronary artery for time step 1.2 s.
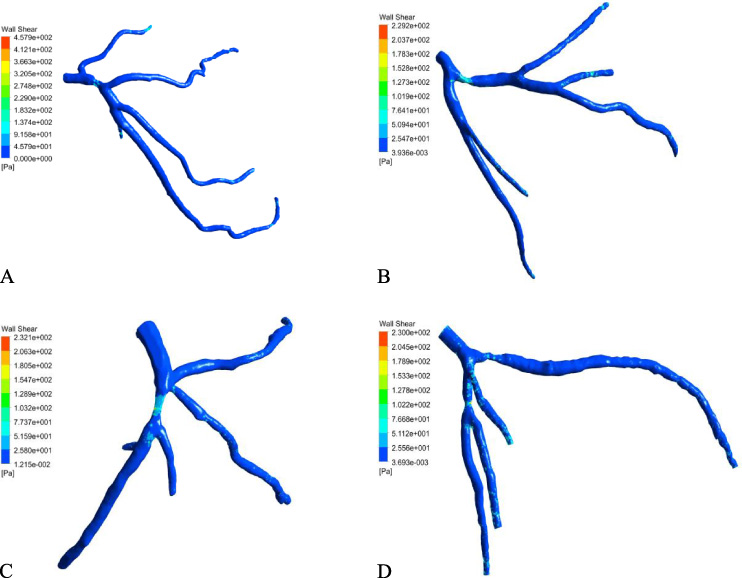
Wall shear stress distribution of four patients in the left coronary artery for time step 1.2 s.
The present study was carried out to analyze the effect of stenosis on the various hemodynamic parameters in 4 suspected patients’ in vivo models. The following conclusion could be drawn from the results with coronary artery disease.
The changes in the hemodynamic parameters would result in corresponding changes in the local blood flow conditions leading to the abnormalities in the coronary arterial conditions. The effect of the stenosis on the pressure variation could lead to the worsening of the atherosclerosis in the patients leading to the complications in the normal functioning of the heart. The high wall shear stress at the stenosis may increase the potential risk of stenosis rupture. The recirculation region at post stenosis could lead to the formation of stenosis.
Footnotes
Acknowledgements
The authors extend their appreciation to the Deanship of Scientific Research at King Khalid University for funding this work through the General Research Project under grant number (G.R.P-246-40).
The authors would also like to thank Sultan Qaboos University for funding the project under Grant No. IG/ENG/MIED/18/03.