
Abstract
Background:
Cigarette smoking is a known risk factor for Alzheimer’s disease (AD). However, the association between neurodegeneration and other substances has not been fully determined. It is of vital importance to evaluate this relationship in populations at high risk of dementia. Since substance use possibly modifies the progression rate of cognitive decline, we studied this association in a unique and well-phenotyped cohort from the University of Antioquia: carriers of the PSEN1-E280A genetic variant.
Objective:
To determine the association between substance use and cognitive decline in carriers of the PSEN1-E280A genetic variant.
Methods:
A retrospective cohort study was conducted with 94 carriers and 69 noncarriers recruited between January 2019 and April 2020. A psychiatrist interviewed the participants using the Consumption of Alcohol, Cigarettes and other Substances questionnaire. The participants were also submitted to cognitive evaluation. The relationship between cognitive decline and substance use was explored through a mixed effects regression model.
Results:
There was an association between cigarettes and better performance on tasks related to perceptual organization, verbal fluency, and memory in carriers. Alcohol had a positive or negative effect on memory according to the type of alcoholic beverage. Results on marijuana use were no conclusive. Coffee was associated with progressive improvements in executive function and verbal fluency.
Conclusion:
Cigarette and alcohol were associated with an improvement of some cognitive assessments, possibly by a survival bias. In addition, coffee was related to improvements in executive function and language; therefore, its short-term neuroprotective potential should be studied.
INTRODUCTION
Research on risk factors for Alzheimer’s disease (AD) has increased significantly in recent years, addressing from apparently nonmodifiable genetic factors to potentially modifiable environmental and lifestyle factors [1, 2]. In developing countries, the important and potentially modifiable risk factors for sporadic AD include cerebrovascular disease (stroke, hypertension, dyslipidemia, hyperinsulinemia, type 2 diabetes, obesity, etc.), negative conditions in childhood (brain development abnormalities, growth retardation, low socioeconomic status, poor environmental enrichment, childhood head trauma, low cognitive reserve), and nutritional factors (diets rich in saturated fat and low in fiber, among other dietary factors) [2–4].
It is well known that substance abuse is associated with accelerated aging, which occurs when biological age exceeds chronological age, causing an older-per-son phenotype to the consumers [5]. Substances such as alcohol, cigarettes and other psychoactive substances catalyze the aging process by a direct cytotoxic effect and by their association with certain risk behaviors and habits such as exposure to sexually transmitted infections or intravenous substance use, limited use of health care services, poor sleep quality, insufficient exercise, and malnutrition [5]. Infections, sleep disorders, sedentary lifestyle, and malnutrition lead to vascular aging and generate neurotoxicity through several mechanisms that truncate cell growth and favor apoptosis [5].
In sporadic AD, low alcohol consumption has been associated with a decreased risk of dementia [6, 7], but a moderate consumption has been related to hippocampal atrophy and a faster decline in lexical flu-ency in cognitive tests [8]. Cigarette smoking has also been associated with cognitive impairment and an earlier AD onset, which is possibly explained by the relationship between smoking and cardiovascular disease, in addition to exposure to the neurotoxins present in cigarettes (RR for dementia 1.6, 95% CI 1.15 –2.20) [2, 9]. Regarding cocaine, different studies have shown that this substance is associated with worse performance in language [10], executive function [11], and memory [11], although there does not seem to be a clear relationship between cocaine use and subsequent risk of dementia. Conversely, can-nabinoids seem to have a neuroprotective role in AD, may be explained by their propensity to reduce glutamatergic transmission, prolong calcium influx, and oxidative stress [12]. Finally, caffeine has also been considered a substance with a possible anti-amyloid effect capable of reducing the extracellular levels of Aβ40/42 and Aβ42 oligomers [13], in addition to rap-idly decreasing the concentration of Aβ42 in plasma after acute administration of this substance [14].
All the above seems to be related to patients with late or sporadic AD, groups of people who frequently show significant differences in disease progression. In contrast, little is known about the possible interactions between substance use and the genetic forms of AD, although some studies suggest potentially important interactions. For example, a recent publication on carriers of the PSEN1-E280A genetic variant suggests that alcohol and cigarette consumption may be related to the rate of cognitive decline in this population [15]. It would be of great interest to know whether individuals with pathological genetic variants with high penetrance have an accelerated or slowed decline due to consumption, which could be reflected in an age of dementia onset different from that of others with a similar genetic risk but without exposure to a certain psychoactive substance. Harwood et al. [16] report that the consumption of two or more alcoholic beverages per day is associated with an onset of dementia 4.1 years earlier than in abstainers (p < 0.05). There were also differences in the age of disease onset among individuals with a history of heavy smoking (smoking ≥1 pack/day), presenting the disease 2.92 years earlier than individuals without this condition. When the presence of three risk factors in the same patient was considered, that is, one or two APOE ɛ4 alleles, in addition to heavy alcohol and cigarette consumption, the age of onset of dementia was reduced by up to ten years compared to that of patients without these conditions. Therefore, substance use emerges as an important modifiable risk factor for both sporadic and familial AD, but more data are needed on how exposure gradually decreases cognitive performance until ending in dementia [6].
This exploratory study investigated the association between the use of alcohol, cigarettes, cocaine, marijuana, and coffee and the progression rate of cognitive decline in carriers of the E280A (Glu280Ala) genetic variant in the presenilin-1 gene, which causes early familial AD and has complete penetrance [17]. We hypothesized that substance consumption modifies the progression rate of cognitive decline in the E280A genetic variant carriers, as in the sporadic forms of AD.
METHODS
A historical cohort design was adopted, taking as the start point for follow-up the date of birth of each of the participants and as the end point the date of patient assessment using for measuring the lifetime consumption (type and amount) of alcohol, cigare-ttes, and other substances. This study followed the ethical guidelines of the Declaration of Helsinki (2013 revision) and resolution no. 8430 of 1993 of the Ministry of Health of the Republic of Colombia, which guarantees the rights of people participating in medical research. Before data collection, this study was approved by the Bioethics in Human Research Committee of the University Research Headquarters (Sede de Investigación Universitaria - SIU) of the University of Antioquia. Participants provided written informed consent before enrollment into the study.
Participants
Individuals 30 years old or older who belonged to a large cohort of 6,000 living members of the PSEN1 E280A kindred, in Antioquia (Colombia) [18, 19], had been genotyped for this mutation, and had undergone a minimum of two to three neuropsychological assessments performed at the Neurosciences Group of Antioquia (Grupo de Neurociencias de Antioquia –GNA). Carriers and noncarriers were invited to participate in the study with the sole objective of maintaining blinding with respect to the genetic status of the asymptomatic participants. Participants could be healthy or be in any of the different stages of the disease, from pre-MCI to dementia. Those with illiteracy or a personal history of stroke, epilepsy, severe head trauma, acquired immunodeficiency syndrome (AIDS), or poorly controlled chronic diseases prior to the onset of dementia due to AD were excluded. Regarding the sample size calculation, given that there is a previously defined cohort with a fixed sample size [15], the statistical power estimates were calculated for effect detection using the formula proposed by Diggle, assuming that with an intraclass correlation coefficient (ICC) = 0.70, an α error = 0.05 for the estimation of a minimum standardized effect of 0.30, with 81 carriers, and 3 or more assessments per individual, the power was 90%.
Randomly, there were 317 individuals from the GNA database (Fig. 1). Of those participants, we could contact just 181 because the rest, 136 candidates, lived abroad or in another city, were part of a clinical trial, passed away, the phone number of inviting them was not available anymore, did not have enough time to participate or, refused to be interviewed. Therefore, we do not know if some traits were relevant to the study, which made those 136 candidates different from the participants. It could mean that the results are not generalizable to the complete set of PSEN1 E280A kindred, turning into a possible source of bias.
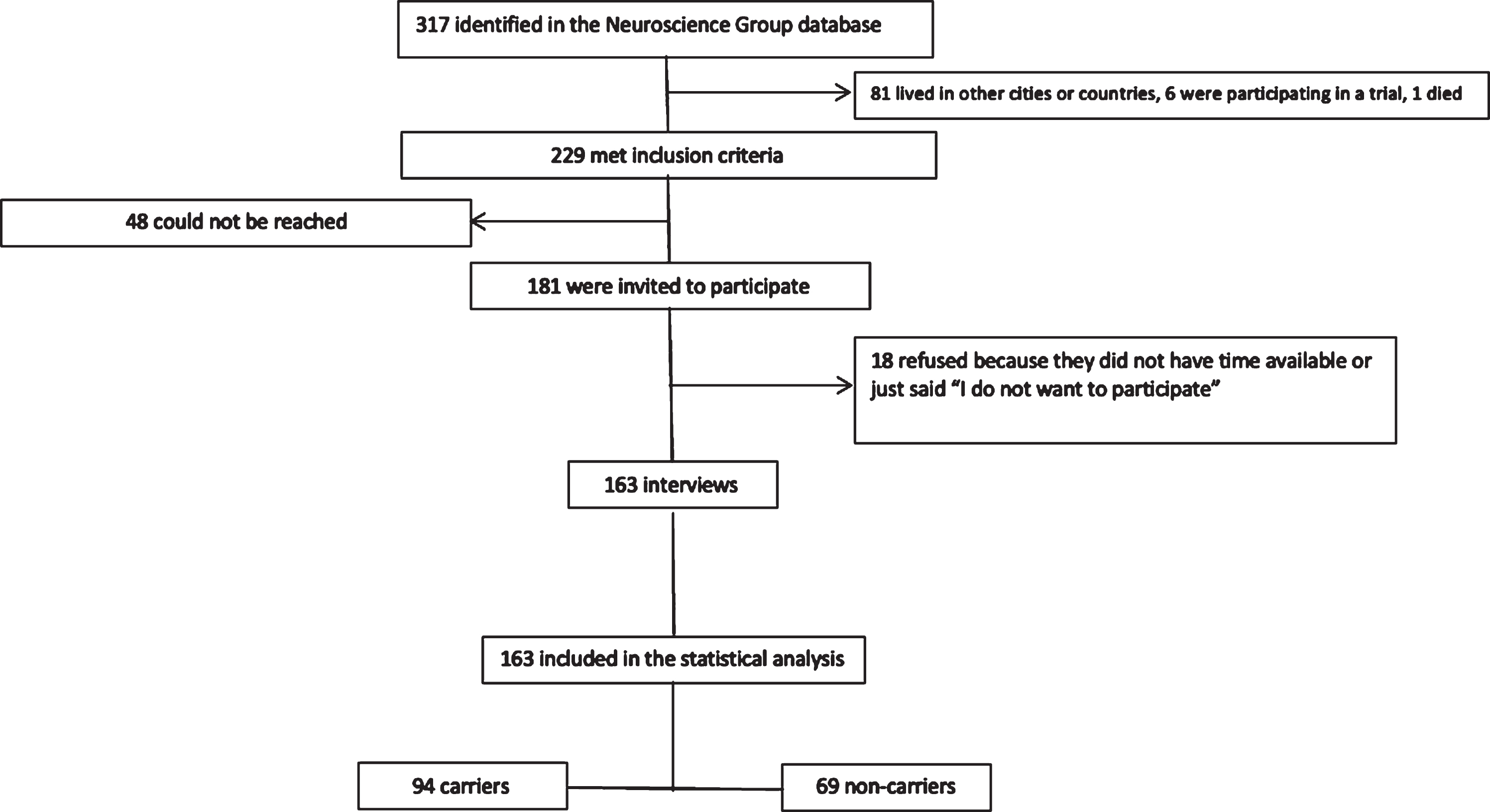
Participants’ selection process.
Data collection
Data were collected between January 25, 2019, and April 29, 2020. Simple random probabilistic sampling was performed for the selection of possible participants; that is, individuals different from the evaluators identified the potential participants from the database of the GNA Information System. For ethical reasons, at no time was the genetic status of any subject revealed to the professionals who conducted the interviews or to the participants.
The selected family members were invited to participate by telephone and were informed about the need to attend a meeting with the researchers to receive complete information about the study. The meeting with each participant was held in one of the GNA facilities or at the home in the case of participants who already had dementia due to AD and were bedridden, and it was the caregiver or a close relative who would provide the patient’s information. The informants of patients with dementia had to be people who had known them well throughout their life, even when they were healthy, that is, without cognitive decline.
A psychiatrist applied the
The presence of mental and behavioral disorders due to alcohol, tobacco, and other psychoactive substances was determined according to the fifth version of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) [20].
For the collection of cognitive data on the selected index subjects, the data previously obtained in the standard neuropsychological assessment batteries at the GNA were reviewed, which included 1) the test battery of the Consortium to Establish a Registry for Alzheimer Disease (CERAD) [21]; 2) the Mini-Mental State Examination (MMSE) [22]; 3) the Subjective Memory Complaints Checklist, applied to both the participant and the informant [21, 23]; 4) the Yesavage scale for depression [24, 25]; 5) the Zung scale for depression [26]; 6) functional scales including the Functioning Assessment Short Test (FAST) [27], Barthel Index [28, 29], Katz Index [30, 31] and Lawton & Brody Scale [32, 33]; and 7) Raven’s Progressive Matrices [34].
CACoS questionnaire
This instrument was developed by the authors to specify the amount, frequency, and severity of consumption of different psychoactive substances, both recently and over the lifetime, which combines elements of four different tools: 1) Inter-American System of Uniform Data about Drug Consumption (SIDUC) [35]; 2) Diagnostic Interview for Genetic Studies, version 3.0 (Spanish version) [36]; 3) Lifestyle: Alcohol use, from the Study for Osteoporotic Fractures (SOF) - Collection Forms; 4) Recommended Alcohol Questions, from the National Institute on Alcohol Abuse and Alcoholism [37]. The time for the administration of the instrument was approximately 1 hour, and it was applied both in the index subject (person who was asked about the amount, frequency, and severity of consumption) and in the companion(s) who agreed to participate in the study. Potential participants with a diagnosis of dementia who still retained their ability to assent but did not accept having a person other than themselves being interview could not participate in the study, given the possibility that the information provided solely and exclusively by them would be unreliable when analyzing the results. In the case of companions of index subjects with severe dementia without the ability to assent, if they agreed to participate, they were interviewed at the GNA facilities, at their home or in a place near it.
To choose the informant of the participants with dementia, some of the recommendations made by Vandeleur et al. to estimate the prevalence of substance use disorders according to family reports were followed [38]: 1) assign a diagnosis if at least 50% of the informants report a positive history for the use of the substance, regardless of how many family members deny history of substance use; 2) ideally interview the partners or children of the index subject; 3) take into account that the female sex in index subjects is associated with a better consensus among informants for all substance use disorders. To explore the interrater reproducibility of the questionnaire, 20 participants and 20 informants were interviewed by telephone or in person by two different investigators (CR and CV). According to Gwet’s AC1, in the interviews, there was a kappa greater than 0.8 for current substance use disorders for cigarettes (kappa 0.95, 95% CI: 0.83–1.0), cocaine (kappa 0.95, 95% CI: 0.83–1.0), and coffee (kappa 0.95, 95% CI: 0.83–1.0) and for previous substance use disorders for cigarettes (kappa 0.94, 95% CI: 0.82–1.0), alcohol (kappa 0.94, 95% CI: 0.81–1.0), and marijuana (kappa 0.95, 95% CI: 0.83–1.0) (data not shown).
Exposure variables
Alcohol drinking was analyzed according to the National Institute on Alcohol Abuse and Alcoholism, NIAAA, which defines heavy drinking as follows: a) for men, consuming more than 14 standard drinks per week; b) for women, consuming more than seven standard drinks per week [39]. The participants were asked about what type of alcoholic drink they used to take along different periods of their lives, and every type of alcohol was measured according to the standard units each one sized as follows 1) beer = 341 mL (12 oz); 2) wine = 150 mL (5 oz); 3) drinks with 40% or higher percentage of alcohol (rum, tequila, aguardiente, whiskey) = 44 mL (1.5 oz) [39].
Smoking was analyzed as a) presence or absence of cigarette consumption throughout life; b) consumption of at least 100 cigarettes throughout life [36]; and c) pack-year index, that was calculated by multiplying the number of packs of cigarettes smoked per day by the number of years the person has smoked [40].
Marijuana and coffee were analyzed as a) presence of absence of the substance consumption throughout life; b) substance (daily use) index, that was calculated by multiplying the number of units of marijuana or coffee per day by the number of years the person has consumed the substance daily; and c) substance (occasional use) index, that was calculated by multiplying the number of units of marijuana or coffee per day by the number of years the person has consumed the substance occasionally.
Neuropsychological assessment
GNA monitors the members of families with AD caused by the genetic variant PSEN1-E280A through medical and neuropsychological assessments. The CERAD test battery used to monitor these families is a Spanish version adapted to the cultural and linguistic idiosyncrasies of this population. This battery has the following sections: 1) verbal fluency; 2) naming; 3) MMSE; 4) word memory; 5) constructional praxis; 6) word recall; 7) word recognition; and 8) line drawing recall [15]. To determine the speed of cognitive decline in both carriers and noncarriers relative to the consumption of different psychoactive substances, the scores of the different tests used by Acosta et al. [21] were analyzed:
Attention
Trail making test, part A (correct answers, errors and test duration) [41, 42].
Memory
Rey-Osterrieth complex figure test (recall, duration of the recall test, retention percentage) [43], word list test (correct answers, recall, word list recognition –“Yes” recognition and “No” recognition) [44], recall of the line drawing test or constructional praxis test –recall [45].
Language
Categorical verbal fluency test for animals [45] and abbreviated Boston naming test (15 items) [45].
Constructional praxis
Constructional praxis test and Rey-Osterrieth complex figure test (copy and duration of the copy test) [43].
Abstract reasoning
Raven’s test (part A) [34].
Executive function
Wisconsin Card Sorting Test (WCST) (correct answers, errors, perseverative errors, categories and conceptual answers) [21] and phonological verbal fluency test [15, 45].
Subjective memory complaints checklist
It is a scale composed of 15 questions about the patient’s current memory. To apply this instrument, it is necessary to interview a family member, who completes the family complaint’s part, and the participant, who completes the patient complaint’s part. The final score is the mean of the sum of the family complaints score and the patient complaints score [23].
Activities of daily living (ADL) assessment
Other tests applied during the follow-up of this cohort were “activities of daily living” assessments as the FAST Scale [27], the Barthel Index [28, 29], the Katz Index [30, 31], and the Lawton & Brody Scale [32, 33]. These tests were administered at the follow-up visits to evaluate the participant’s cognition and functionality.
Statistical analysis
The reproducibility of the CACoS questionnaire was evaluated by measuring the kappa, weighted kappa, and Lin correlation coefficients. The sociodemographic characteristics of the population were described by frequencies and percentages for the qualitative variables and measures of central tendency and dispersion for the quantitative variables after testing the data distribution using the Shapiro-Wilk test and visual scanning of normality plots. Age was centered at 20 years to be able to interpret the intercept, that is, to know what the expected score would be in the cognitive or functional variable of interest, assuming that individuals began to be observed after the age of 20. To explore the possible associations between the lifetime consumption of different psychoactive substances and the progression rate of cognitive decline in carriers of the mutation, a mixed effects regression model was used, using the lmer function of the lme4 package [46]. Given that previous studies support the assumption that cognitive decline is not a constant linear process [15], a quadratic term was included to explore curvilinear behavior in cognitive decline. A random intercept model was adopted (centered at 20 years for ease of interpretation), considering that there are variations in the initial cognitive level among individuals; a random coefficient associated with cognitive decline was not included given the heterogeneity and limitations in the number of assessments among patients; the effect of all substance use-related variables and their interaction with time (chronological age at which the assessment was performed) was included as a fixed effect to evaluate changes in the rate of cognitive decline, under the hypothesis that some patients may have a more rapid, stable or slow progression in behavior on the evaluated cognitive tasks. Although each variable was analyzed through a linear model, some variants were transformed to a beta-binomial model as a sensitivity analysis: MMSE, Boston Naming Test, Word List Recall, Word List Recognition, Constructional Praxis, Constructional Praxis Recall, and WCST Categories (see Supplementary Material). The 95% confidence interval (95% CI) was included for each coefficient, and all analyses were performed with the statistical software R version. 4.0.5 [47] and RStudio [48].
RESULTS
Figure 1 illustrates the participant selection process. A total of 317 potential participants who met the inclusion criteria were identified in the GNA database. Of this group, 81 people lived in other cities or countries, 6 were participating in another study of the group, which prevented them from participating in this study, and one subject had died. Of the 229 remaining subjects, 181 were contacted. Of the latter group, 18 refused to participate due to lack of time or other reasons that they did not share with the investigators.
Of the 163 people who agreed to participate in the study, 94 were carriers of the PSEN1-E280A genetic variant (Table 1). The mean age of the carriers was 40.8 years, and the median age was 37.5 years. The mean number of years of schooling in this group was 9.31, with a median of 11.0 years. Of the 94 carriers, there were 36 individuals with some degree of cognitive impairment, whether it was MCI or dementia. Table 2 shows information on the lifetime consumption of different psychoactive substances in carriers.
Demographic traits of the PSEN1 E280A carriers
*Job in people with dementia refers to the job before the cognitive impairment onset. MCI, mild cognitive impairment.
Substance consumption throughout life of the PSEN1 E280A carriers
*Pack-year index, No. of packs of cigarettes smoked per day times No. of years the person has smoked. Marijuana index, number of units per day times number of years of consumption. Coffee index, number of units per day times number of years of consumption. AAO, age at onset.
CACoS interview
According with Gwet’s AC1, there was an agreement > 0.8 for a current consumption disorder of substances as cigarette, cocaine, and coffee (0.95, CI95% 0.83–1.0); and for a previous consumption disorder of cigarette (0.94, CI95% 0.82–1.0), alcohol (0.94, CI95% 0.81–1.0), and marijuana (0.95, CI95% 0.83–1.0).
History of lifetime substance consumption and decline rate
There was an interaction between smoking more than 100 cigarettes throughout life and age in the perceptual organization evaluated by the Rey-Osterrieth complex figure copy, producing an increase of 0.595 points/year among carriers who smoke versus nonsmoking carriers (95% CI 0.050–1.140), and in the Reisberg FAST score, producing a decrease of 0.219 points/year among smokers versus nonsmokers (95% CI –0.362––0.076) (Table 3).
Effects of alcohol, cigarette, marijuana, and coffee on the cognitive profile of the PSEN1 E280A carriers (linear regression model), adjusting for age and schooling
MMSE, Mini-Mental State Examination; WCST, Wisconsin Card Sorting Test; SMC, Subjective Memory Complains; FAST, Functioning Assessment Short Test.
For alcohol, only one statistically significant ass-ociation was observed between drinking > 7 units/week for women or > 14 units/week for men when the carriers were 19 to 40 years old, and age. Specifically, in the Barthel index, the interaction between alcohol consumption and age increased by 1.472 points/year among carriers who drank more than 7 or 14 units versus carriers who did not (95% CI 0.708–2.237) (Table 3).
Regarding a history of lifetime marijuana consumption, on the categorical verbal fluency test for animals, an interaction between marijuana consumption and age was evidenced, producing an increase of 0.375 words/year among carriers who consumed marijuana at some point in life versus carriers who did not consume marijuana (95% CI –0.007 –0.757) (Table 3).
An interaction between marijuana consumption and age was also observed on the Rey-Osterrieth complex figure. Regarding the retention percentage, there was an interaction between marijuana consumption and age, producing an increase of 2.614% of retention among carriers who consumed marijuana at some point in life versus non consuming carriers (95% CI 0.431–4.798) (Table 3).
Last, regarding some stimulant substances, it was found that, unlike cocaine, for which there were no significant interactions, coffee seems to favor performance on the categorical verbal fluency test for animals and on the WCST. On the categorical verbal fluency test for animals, an increase of 0.313 words/year (95% CI –0.020–0.646) was observed among carriers who consumed coffee daily throughout the lifetime. Regarding conceptual answers on the WCST (correct responses in groups of 3 or more), an increase of 0.950 points/year (95% CI 0.128–1.772) was observed among carriers who consumed coffee daily throughout the lifetime versus no consumers (Table 3).
Relationship between amount consumed and decline rate
Although the amount consumed * follow-up time interaction coefficients were very small for carriers of the PSEN1-E280A variant in all cases, the results suggest some cognitive effect of different psychoactive substances. For example, regarding the consumption of aguardiente (a sugarcane spirit) between 19 and 30 years of age, the following was evidenced for the word list test –correct answers: for each additional unit of aguardiente consumed in this age range, and for each year of life, there was an expected increase of 0.023 points on this test (95% CI 0.003–0.044). This figure, although statistically significant, is very small, which suggests that a significant number of years of follow-up or a certain number of units of aguardiente would be required to observe a relevant effect from the clinical standpoint. The same could be argued for the consumption of aguardiente between 19 and 30 years for the word list test –recall (observed estimate 0.011 points, 95% CI 0.001–0.021) and for the consumption of aguardiente at age above 30 years on the word list test –correct answers (observed estimate 0.034 points, 95% CI 0.008–0.060). Rum consumption of seems to have an opposite effect, such that, on the MMSE, for each additional unit of rum consumed between 19 and 30 years, and for each year of life, there is an expected decrease of 0.027 points on this test (95% CI –0.053––0.001). A similar effect of rum consumption was also observed in those younger than 30 years for the categorical verbal fluency test for animals (observed estimate –0.036, 95% CI –0.066––0.006) and in those older than 30 years on the MMSE (observed estimate –0.029, 95% CI –0.057––0.001). No significant interactions were observed with beer.
Regarding cigarette consumption, two pack-year indices were calculated: one for usual cigarette consumption and another for the maximum number of cigarettes consumed in a day. Regarding the “usual” consumption of cigarettes, the categorical verbal fluency test for animals showed the following: for each one-unit increase in the pack-year index among carriers, and for each year of life, there was an expected increase of 0.031 points on this test (95% CI 0.003–0.058). Regarding the word list memory test, an interaction between cigarette smoking and age was evidenced, producing an increase of 0.030 words/year among carriers who smoke versus nonsmoking carriers (95% CI 0.005–0.054). Although these figures were statistically significant, they are very small, which suggests that a significant number of years of follow-up or some increase in the number of packs-year would be required to observe a relevant effect from the clinical standpoint. Similar results were obtained for the maximum number of cigarettes per day on the word list test –correct answers (observed estimate 0.024, 95% CI 0.007–0.042), word list test –recall (observed estimate 0.009, 95% CI. 0.001–0.018), and constructional praxis test –recall (observed estimate 0.016, 95% CI 0.005–0.027) tests.
With respect to marijuana, a consumption index was calculated as follows: number of units of can-nabis consumed in one day *number of years of consumption. This calculation was made for two scenarios: daily marijuana use, and occasional marijuana use. The analysis with daily consumption did not show statistically significant results. However, with respect to the “typical” occasional consumption, it was observed that, for each one-unit increase in the cannabis units-year index among carriers, and for each year of life, there is an expected increase of 0.111 points in the word list test –correct answers (95% CI 0.032–0.191).
Finally, for coffee, a consumption index was calculated as follows: number of cups of coffee consumed in a day * number of years of consumption. Regarding daily coffee consumption, there was an increase in the scores of the MMSE (observed estimate 0.003, 95% CI 0.001–0.006) and of the categorical verbal fluency test for animals (observed estimate 0.003, 95% CI 0.000–0.007). However, occasional coffee consumption was associated with the opposite effect, that is, a decrease in the scores on categorical verbal fluency test for animals (observed estimate –0.015, 95% CI –0.028––0.002), word list test –correct answers (observed estimate –0.014, 95% CI –0.026––0.003), and word list test –recall (observed estimate –0.008, 95% CI –0.014––0.002) tests.
DISCUSSION
In this study, an association between cigarette, alcohol, marijuana, and coffee consumption with the progression rate of cognitive decline was observed in carriers of the PSEN1-E280A (Glu280Ala) genetic variant. Daily coffee consumption was associated with a possible protective effect on the progression of cognitive decline over time, as was alcohol consumption. Cigarettes, alcohol, and marijuana also showed a positive impact on the performance of certain language and memory tasks. For cocaine use, no association was observed, although this result is possibly explained by the low prevalence of cocaine use in this sample of patients. All these results should be interpreted with caution, given the exploratory nature of this study.
Smoking more than 100 cigarettes throughout life was associated with better performance on the Rey-Osterrieth complex figure copy, a test for perceptual organization. Moreover, cigarette smoking seems to have a positive effect on language assessments such as the verbal fluency test and on memory according to the results observed in the word list memory and recall and praxis recall tests. Nevertheless, these findings may be explained by the survival bias found in other studies, in which there was an apparent positive effect of smoking on cognition, or by the stimulating effect on the central nervous system, which perhaps initially correlates with an improvement in the performance of the tests for some years but that later could lead to an acceleration of cognitive decline [9, 50]. For example, Almeida et al. [49] published a meta-analysis of case-control and cohort studies. In case-control studies, they found a pooled OR adjusted for age, sex, schooling, and alcohol use of 0.82. On the other hand, the overall relative risk (RR) of AD calculated for cohort studies was 1.10 and restricting the analysis to the two cohort studies which described the number of smokers at baseline that later were diagnosed with dementia, RR was 1.99. These conflicting results about the direction of the association between smoking and AD could be explained by an apparent improvement of some cognitive domains, but earlier AD onset and premature death among certain smokers who were not as good at repairing their DNA as the surviving cigarette smokers used to make comparisons with an age-matched nonsmokers’ group [50, 51]. Therefore, although the smoker carriers of the present study had better performance in some tests than nonsmoker carriers, it does not possibly mean that smoking protects against AD [9, 50].
Indeed, a large cohort study showed that the risk of dementia and AD is dose-dependent: the risk increases with the increasing number of cigarettes consumed [52]. Another study, which investigated the effects of alcohol and cigarettes on the age of onset of AD, found that individuals who smoked more than one pack of cigarettes per day were diagnosed 2.5 years before nonsmokers (p < 0.05) [16]. The key mechanism behind the deleterious effect of cigarettes on cognition, associated with the increased risk of AD, consists of neuroinflammation with oxidative stress, as suggested by the results of the recent study published by Liu et al., which found a positive association between the levels of Aβ42 and tumor necrosis factor alpha (TNFα) in people who smoke at least 20 cigarettes per day [53]. Apparently, smoking affects the immune system, increasing the production of TNFα, which leads to an increase in the load of amyloid-β through a greater production of β-secretase [53]. Moreover, in 2019, Pan et al. published a meta-analysis about the relationship between smoking and stroke, a contributing factor for cognitive impairment in our patients. They show an increased risk of stroke in smokers versus nonsmokers, with a pooled OR of 1.61 (95% CI 1.49–2.48) [54]. The mechanisms behind this relationship are increased levels of homocysteine and fibrinogen, atherosclerosis, and oxidized low–density lipoprotein cholesterol, besides the higher risk of atrial fibrillation, diabetes, hypertension, and resting sinus tachycardia [6, 54].
The U.S. Department of Health and Human Services defines heavy drinking as consuming more than 14 standard drinks per week for men, and more than 7 standard per week for women [39]. Different from expected, there was a positive effect of heavy drinking on the Barthel index for activities of daily living. This finding may be explained by a selection bias [55]. For instance, as Naimi et al. mentioned in an article about selection biases on studies related to alcohol consumption [55], healthier drinkers, more resilient drinkers, or less risky drinkers would tend to be over-represented in observational research, and those with risky consumption patterns or an alcohol-related disorder might be less likely to be included in studies. Therefore, drinkers who do not participate could have more alcohol-related problems than drinkers who participate in interviews and surveys. Possibly, drinking carriers would be more functional in basic activities of daily living or have a better Barthel index than nondrinking carriers for the same traits as they agreed to be enrolled, and these characteristics might be the real reasons for their higher functionality, but not the alcohol consumption itself.
When the association between alcohol and rate of cognitive decline was evaluated by the type of alcoholic beverage, although there was no association with beer, aguardiente—a drink commonly consumed in Colombia—was related to an expected increase in the score of tests such as word list memory and recall. Rum had an opposite effect, negatively impacting the score on the MMSE and verbal fluency test between 19 and 30 years of age. However, it is not possible to determine with these results whether there is a cutoff point for the units of these two classes of alcohol after which the apparent protective effect of aguardiente is lost or the possible deleterious effect of rum is further enhanced. Ruitenber et al., in a prospective cohort study with 7,983 participants, of whom 197 individuals developed dementia, found an association between light to moderate alcohol consumption (one to three drinks per day) and a lower risk of developing dementia (hazard ratio [HR] 0.58, 95% CI 0.38–0.90), although unlike the present study, they did not find a difference in the association according to the type of alcoholic beverage [56]. Other studies have also reported a protective effect of moderate alcohol consumption with respect to the risk of developing dementia [57, 58].
Other studies report a negative impact of alcohol on the time of onset and progression of dementia, even if considered moderate. For example, Harwood et al. found that individuals who consumed more than two drinks a day had an age of onset 4.1 years earlier than those without a history of consumption [16]. In turn, in 2017, Topiwala et al. published a study in which they reported that the consumption of more than 30 units of alcohol per week was associated with a high risk of hippocampal atrophy (OR 5.8, 95% CI 1.8–18.6), in addition to a faster decline in semantic fluency, without being able to demonstrate a protective role for light alcohol consumption [8].
Different studies have shown the association between alcohol and contributing factors of neurodegeneration as stroke. For instance, in 2014, Zhang et al. published a meta-analysis of prospective studies of alcohol intake and risk of stroke, and they found that low alcohol intake is associated with a reduced risk of stroke morbimortality, whereas heavy alcohol intake is associated with an increased risk of stroke [59]. In 2016, Larsson et al. found that the association between alcohol and stroke types depended on the quantity of consumption: light and moderate consumption were inversely associated with ischemic stroke, and heavy drinking was associated with a high risk of all stroke types, mainly with hemorrhagic strokes [60]. The possible underlying mechanisms of alcohol as a stroke causative are functional impairment of vascular endothelium, inflammation, atrial fibrillation, and high blood pressure [61].
Similarly to cigarettes, lifetime marijuana consumption positively impacted cognitive assessments such as the Osterrieth complex figure –retention percentage. Despite that, not a daily but a “typical” occasional use of this substance, that is, of the average units of marijuana per day of consumption, was related to a positive impact on the word list memory test score over time. This finding can be explained by the dual, age-dependent and paradoxical effects of the endocannabinoid system in the regulation of memory and learning: the use of marijuana affects memory and cognition in young people [62], and predisposes to transient ischemic attacks and ischemic stroke [63, 64], but it has been observed that chronic, low-dose tetrahydrocannabinol or cannabis extracts can slow or even reverse cognitive decline in old age [12, 62]. This result could also be due to factors not measured in the study, related to the occasional use of marijuana (daily consumption did not yield any significant result).
Cocaine was not related to an effect on neuropsychological tests in this study, although a deleterious effect of this substance on brain well-being has been described, associated with a worse performance on the assessment of cognitive skills such as language [10]. However, the study by Blanco-Presas et al. concluded that chronic cocaine abuse does not seem to be associated with cognitive impairment greater than that attributed to concomitant abuse of cocaine and alcohol [11].
In the present study, a positive effect of lifetime coffee consumption was found on the evolution of scores on tests such as the verbal fluency test and WCST. The protective effect seems to be more closely associated with daily consumption compared to the occasional use of this substance. Indeed, some studies, such as that of Lindsay et al., have shown that, among other factors, coffee consumption seems to reduce the risk of AD [57]. Among the mechanisms possibly associated with the protective effect of coffee are inhibition of the adenosine receptor, reduction of the risk of type 2 diabetes, and inhibition of amyloid-β protein precursor cleavage enzyme 1 (BACE-1), and the neuroprotective effect that other coffee components, such as trigonelline [13] and theobromine [65] may have. This protective effect of coffee seems to depend on the frequency and amount of consumption, which could explain why the protective effect of coffee in this study was observed for daily consumption and not for occasional consumption [13].
This study has several weaknesses. First, this is an exploratory study in which there was a small sample size. With small samples, the estimators may be initially biased by chance (under the probabilistic sample assumption). Additionally, due to this limitation, it was not possible to control for other factors that could confound the effect of each of the substances on cognitive decline, such as sex, education, socioeconomic status, or the concomitant use of different drugs. It is also difficult to know whether there were sociodemographic differences and differences in the presence and characteristics of consumption between the people who agreed and did not agree to participate in the study. Last, the measurement of consumption depended exclusively on what the participants wanted to and could report, which makes some biases, such as the memory and social desirability (participant omits certain information for fear of being judged negatively by the evaluator) biases inevitable. To attempt to mitigate the latter, the participants were asked permission to interview another person who knew them well and could provide information about their pattern of consumption, although this could not completely control the recall bias.
The strengths of the study include the design of an instrument exclusively for the measurement of exposure, the CACoS questionnaire. This instrument not only considered the presence or absence of a substance use disorder but also the amount and frequency of consumption throughout the life of the participant. The evaluators were previously trained before the administration of the instrument and remained blinded to the carrier status of the gene causing AD in this population.
In conclusion, the consumption of cigarettes was associated with an improvement of some cognitive assessments, finding that could be explained by a survival bias. Alcohol seems to have impact on the rate of cognitive decline, determined by the type of alcoholic beverage consumed by the study participants. Further studies with larger samples and on carriers of other genetic variants are required to verify the external validity of this result. Occasional use of marijuana was associated with a positive impact on memory. However, the quantity and frequency related to “occasional” use are entirely unknown. Coffee seems to be associated with a slowing of the decline of cognitive skills such as memory and executive function. This finding suggests the importance of continuing to investigate the possible neuroprotective role of the different coffee components in the near future.
Footnotes
ACKNOWLEDGMENTS
We acknowledge the PSEN1-E280A families for contributing their time and effort. In addition, we acknowledge Liliana Hincapie and Francisco Pie-drahita for their efficient work during the recruitment period. Lastly, we acknowledge Alzheimer’s Association, AA, Global Brain Health Institute, GBHI, and Alzheimer’s Society United Kingdom for their generous financial contribution and academic support, without which this study would not have been possible.
This study was supported by grant GBHI ALZ UK–19–592004 from the Global Brain Health Institute, the Alzheimer’s Association and the Alzhe-imer’s Society Pilot Awards for Global Brain Health Leaders.