
Abstract
Background:
Multiple sclerosis (MS) is a prototype neuroinflammatory disorder with increasingly recognized role for neurodegeneration. Most first-line treatments cannot prevent the progression of neurodegeneration and the resultant disability. Interventions can improve symptoms of MS and might provide insights into the underlying pathology.
Objective:
To investigate the effect of intermittent caloric restriction on neuroimaging markers of MS.
Methods:
We randomized ten participants with relapsing remitting MS to either a 12-week intermittent calorie restriction (iCR) diet (n = 5) or control (n = 5). Cortical thickness and volumes were measured through FreeSurfer, cortical perfusion was measured by arterial spin labeling and neuroinflammation through diffusion basis spectrum imaging.
Results:
After 12 weeks of iCR, brain volume increased in the left superior and inferior parietal gyri (p: 0.050 and 0.049, respectively) and the banks of the superior temporal sulcus (p: 0.01). Similarly in the iCR group, cortical thickness improved in the bilateral medial orbitofrontal gyri (p: 0.04 and 0.05 in right and left, respectively), the left superior temporal gyrus (p: 0.03), and the frontal pole (p: 0.008) among others. Cerebral perfusion decreased in the bilateral fusiform gyri (p: 0.047 and 0.02 in right and left, respectively) and increased in the bilateral deep anterior white matter (p: 0.03 and 0.013 in right and left, respectively). Neuroinflammation, demonstrated through hindered and restricted water fractions (HF and RF), decreased in the left optic tract (HF p: 0.02), and the right extreme capsule (RF p: 0.007 and HF p: 0.003).
Conclusion:
These pilot data suggest therapeutic effects of iCR in improving cortical volume and thickness and mitigating neuroinflammation in midlife adults with MS.
Keywords
INTRODUCTION
Multiple sclerosis (MS) is an autoimmune inflammatory demyelinating disease of the central nervous system with hallmark axonal and neuronal injury and neuroinflammation [1]. Beyond the inflammatory white matter (WM) pathogenesis, there is a clear role of grey matter (GM) atrophy in MS that correlates with WM atrophy in early disease, only to progress independently in the later stages [2, 3]. Unfortunately, most first-line disease-modifying treatments cannot prevent the progression of neurodegeneration and the resultant disability over time [4, 5]. Dietary habits and nutritional deficiencies have long been implicated in the risk of MS [1 , 6–8]. Indeed, MS is found to be associated with childhood and adolescence obesity, a risk attributed to chronic inflammatory state induced by obesity [1, 8]. Similarly, vitamin D deficiency is a known risk factor for MS and implicates faster progression of disability in these patients [6, 7].
Dietary interventions can improve brain function and even prevent or treat brain disorders [9, 10]. Chronic caloric restriction (CR) and intermittent fasting are mainstay mechanisms by which altering dietary intake can improve brain health [11]. Both of these dietary strategies improve cognition in older adults and prevent cognitive decline in preclinical Alzheimer’s disease (AD) [11 –13]. In addition, a growing body of evidence suggests intermittent fasting can improve fatigue and emotional well-being and mitigate the peripheral inflammatory response in patients with MS [14 –17]. Diets based on intermittent fasting paired with mild CR are easier to maintain compared to those based on daily CR and therefore more commonly used when studying the health benefits of fasting. Our group has previously shown that chronic CR and intermittent fasting diets can ameliorate inflammation and demyelination in MS animal models, while reducing the number of circulating pro-inflammatory B-cells and CD4+ T-cells in patients with MS [18, 19]. Whether these changes translate to alterations in imaging biomarkers of MS is yet to be investigated.
Here we report results of the first human study investigating changes in neuroimaging biomarkers of MS including; 1) brain volumetric measurements; 2) relative regional perfusion, 3) neuroinflammatory markers, and 4) lesional WM volume, following a 12-week intermittent CR (iCR) diet in MS patients. Findings from this study would inform on possible dietary interventions to prevent disease progression in MS and neurodegenerative disorders such as AD.
METHODS
Participants
Participants enrolled in this study represent a subset of participants (n = 10; 8 women and 2 men) who were enrolled in a randomized, controlled, single-blinded clinical trial (Clinicaltrials.gov number NCT03539094) in which 42 individuals with relapsing remitting MS were recruited consecutively from referrals to the John L. Trotter MS center at Washington University School of Medicine in St. Louis. These individuals were randomly assigned to either the 12-week iCR intervention or a non-intervention control group who consumed a standard western diet. Participants in this study completed non-contrast brain magnetic resonance imaging (MRI) studies at baseline and at 12 weeks after the intervention.
Participants were eligible to participate in the study if, at the time of enrollment, they: 1) were diagnosed with relapsing remitting MS based on the 2017 McDonald criteria [20]; 2) were untreated for 6 months preceding the baseline visit or on a stable dose of standard disease modifying treatments for the past 3 months; 3) were not experiencing a relapse; and 4) had an Expanded Disability Status Scale (EDSS) score lower than 6.0. Exclusion criteria included having a history of smoking, any other chronic disease (excluding MS) or conditions that could interfere with the study and interpretation of results (e.g., diabetes, eating disorders, corticosteroid treatment) in the month prior to the baseline visit, or being on a special diet and not willing to stop at least one month prior to baseline visit.
Dietary intervention and metrics
All participants were consuming a standard western diet at the time of recruitment which is believed to be low in fruits, vegetables, whole grains, and legumes and high in fat, sugar, sodium and ultra-processed foods [21]. After completing all baseline testing, participants in the iCR group were instructed to reduce their daily calorie intake to ∼25% of usual intake on two non-consecutive days per week. On these “fasting” days, participants were allowed to eat one or two salads consisting of fresh or steamed non starchy vegetables with a light dressing and were asked not to exceed 500 calories/day. In addition, they were advised not to overcompensate on non-fasting days. This dietary regimen ultimately resulted in approximately 20% total caloric restriction on a weekly basis [18]. Participants in the control group had unsupervised access to food and were instructed to maintain their habitual diet.
Participants were asked to record their usual food and drinks intake for 4 consecutive days (2 weekdays and 2 weekend days including one fasting day for the iCR group) at the baseline, 6-week and 12-week visits. A study dietitian contacted the participants every week by email or telephone to check their intake diaries and to provide motivational support and advice for participants undergoing fasting. Intake diaries were analyzed to determine nutrient intakes using the NDSR program (Nutrition Data System for Research from the Nutrition Coordinating Center at the University of Minnesota), version 2017 to version 2021.
Brain structural, perfusion and diffusion MR imaging
All scans were acquired on a Vida 3T scanner with 1.0×1.0×1.2 mm3 resolution using the Alzheimer’s Disease Neuroimaging Initiative (ADNI) protocol [22]. These included T1 weighted (T1w) magnetization-prepared 180 degrees radio-frequency pulses and rapid gradient-echo (MPRAGE) with 1.0×1.0×1.2 mm3 resolution, followed by a 3D pseudo continuous arterial spin labeling (ASL), a 3D Fluid attenuated inversion recovery (FLAIR) scan and diffusion basis spectrum imaging (DBSI) images. Volumetric quantification was performed on T1w images using automated FreeSurfer 7.1.1 segmentation generating absolute volumes for 68 cortical and 8 subcortical structures and average thickness of 68 cortical regions [23]. Relative regional blood flow (rCBF) were obtained using the ASL scans and through the ASL-MRI-cloud [24]. Finally, diffusion-weighted images were collected at 2×2×2 mm3 resolution using a hybrid 82-direction diffusion encoding scheme with multiple diffusion weightings and a maximum b-value of 1500 s/mm2. DBSI metric maps were processed using the Diffusion Histology Imaging (DHI) package, an in-house MATLAB® based tool in which a multiple-tensor modeling approach is used to describe the anisotropic axonal fiber and a full-range of the isotropic components of the surrounding environment [25, 26]. This generates DBSI metrics such as hindered diffusion fraction (HF), restricted diffusion fraction (RF), and isotropic free water fraction (WF), as well as conventional diffusion metrics such as fractional anisotropy (FA), axial, radial and mean diffusivities (AxD, RD, and MD). Finally, FLAIR and T1w images were used to automatically segment and quantify WM lesions volume through the lesionBrain pipeline within the volBrain set of online brain imaging tools [27]. Absolute and normalized lesion volumes as well as the lesion burden—lesion volume divided by the WM volume—were extracted from the reports.
Statistical analyses
Statistical analyses were performed using the R software version 4.0.5. The Mann-Whitney U was used to compare caloric intake of participants in their baseline, while the Wilcoxon signed-rank test was used to compare caloric intake on fasting versus non-fasting days during the 6th and 12th weeks. The package lme4 and function lmer were used to model changes in imaging markers as a function of time (baseline versus week 12) and treatment group (control or iCR). p-values of the time*treatment interaction term were corrected for multiple comparisons through the Benjamini-Hochberg method to reduce the false-discovery rate. Partial eta-squared (
RESULTS
Participants were all right handed, aged between 35–64 years old (mean±SD: 46±10), and their body mass index (BMI) at baseline ranged from high normal to obese (median (IQR) = 30 (24–35)). Those randomized to the iCR and control group did not differ in their average age and BMI (p-value of all comparisons >0.05, Table 1). Individuals in the iCR group lost about 2.1% to 6.2% of their total body weight, while the controls weight change ranged from losing 0.11% to gaining 0.9% of their baseline body weight over a period of 12 weeks (Supplementary Table 1). Supplementary Table 2 demonstrates the average caloric intake of participants in the iCR and control groups at baseline and during intervention. Average caloric intake of participants in the two groups were not different at baseline. Importantly, caloric intake of iCR group in their non-fasting days during the 6th and 12th week assessments were not different from their baseline or the caloric intake of the control groups during the same period (p-values of all tests >0.05).
Clinical and demographic features of the study groups
iCR, intermittent caloric restriction; IQR, interquartile range; Control, standard Western diet; BMI, body mass index; EDSS, Expanded Disability Status Scale.
Comparing volumetric changes in 68 cortical and 8 subcortical regions in both hemispheres revealed a borderline significant relationship between iCR treatment and increase in cortical volume in the left inferior (F(2, 10): 6, p: 0.055,
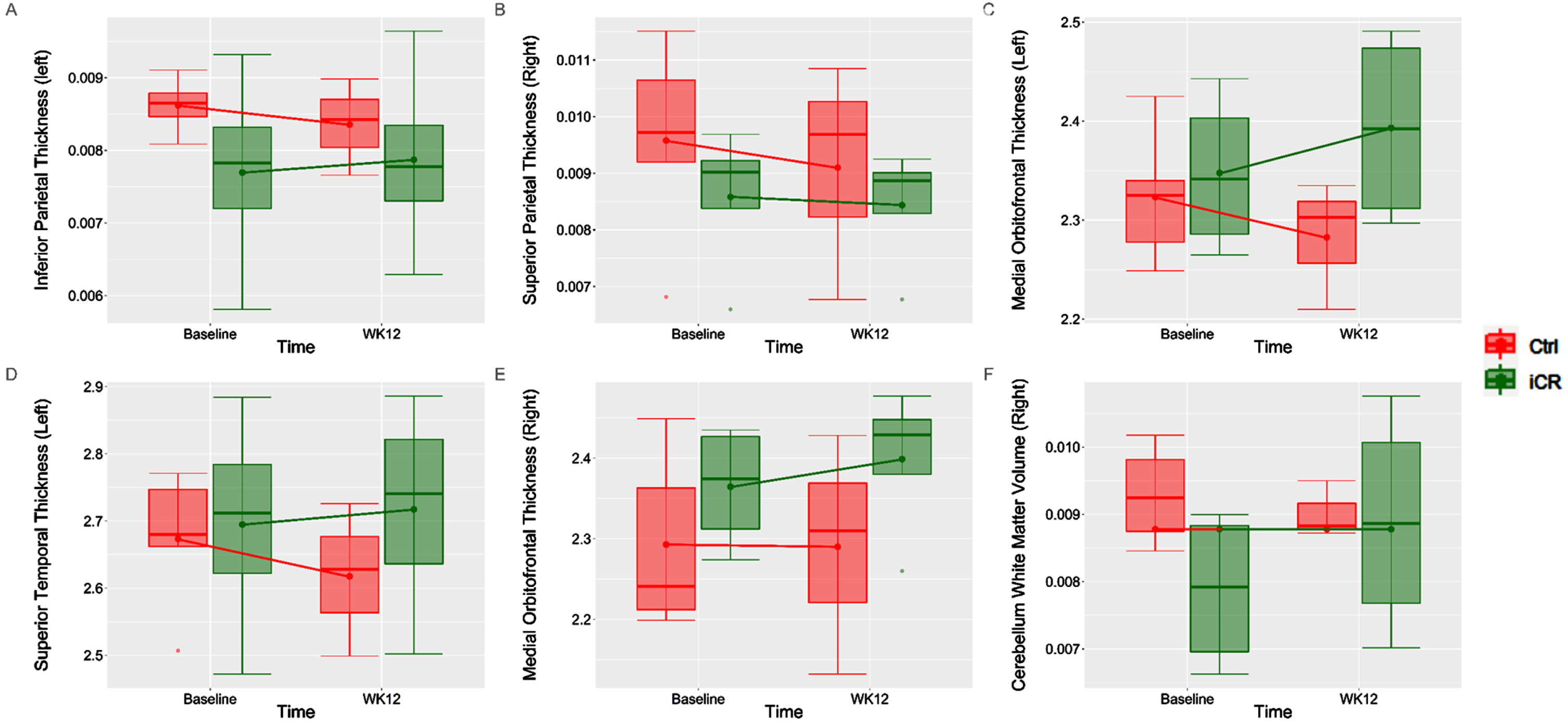
Changes in cortical and subcortical regional thickness/volume from baseline to week 12 in the intermittent calorie restriction and control groups. iCR, intermittent caloric restriction group; Ctrl, control (standard western diet) group.
Changes in investigated variables from baseline to week 12 between the treatment groups
iCR, intermittent caloric restriction; EMM, estimated marginal means; 95% CI, 95% confidence interval; rCBF, relative/regional cerebral blood flow as percentages; DBSI, diffusion basis spectrum imaging; volume, normalized cortical volumes as percentages; thickness, cortical thickness in mm.
When change in the rCBF was compared between the baseline and 12-week visits, perfusion increased in the bilateral fusiform gyri (F(2, 10): 32, p: 0.047,
When DBSI changes were compared in the WM, iCR diet was directly related to changes in FA (F(2, 10): 34, p: 0.04,

Changes in diffusion basis spectrum imaging metrics from baseline to week 12 in the intermittent calorie restriction and control groups. iCR, intermittent caloric restriction group; Ctrl, control (standard western diet) group.
No changes were observed in WM lesion volume or lesion burden in the iCR group after 12 weeks of dieting compared to those following a standard western diet. Supplementary Tables 3–5 demonstrate significance levels for the time and time*treatment interaction terms for volumetric, perfusion and DBSI models across all investigated regions.
DISCUSSION
Evidence from animal studies support a role for CR in reduction of neuroinflammation and preservation of brain oxidative metabolism, vascular endothelial function, blood flow, and brain volume with aging [28 –31]. Human studies are nonetheless significantly limited and focused mostly on the effect of CR or CR mimicking diets in clinical improvement of various neurological disorders [11, 32].
Understanding of AD pathology is changing from the historic focus on amyloid and tau to a greater recognition of neuroinflammation as part of this disorder [33]. Both MS and AD share common molecular mechanisms for inflammation including: 1) activation of astrocytes and microglia, 2) secretion of inflammatory cytokines and chemokines, and 3) recruitment of peripheral immune cells into the brain [34, 35]. Adolescence and midlife obesity are examples of pro-inflammatory conditions that are known risk factor for MS and AD respectively [1, 36]. Similarly, and given its immunomodulatory role, deficiency in vitamin D is associated with increased incidence of MS and faster disease progression, with similar but less strong evidence connecting it to AD risk [6 , 37]. Additional key pathological players common to both disorders are atrophy and hypoperfusion in the non-lesional WM as well as the GM, both being related to long-term disability and cognitive decline in these patients [38 –40]. Similarly to MS, AD therapeutics have also been limited in preventing GM and WM atrophy, progression of neurodegeneration, and the resulting cognitive decline [41, 42]. Thus, MS may act as a model of understanding neuroinflammation and to some extent neurodegeneration, including the testing of new dietary treatments.
We found volumetric benefits from the iCR in regions implicated in MS atrophy. While atrophy is a known biological substrate of neurodegenerative disorders such as AD, MS is increasingly noted for cortical atrophy patterns that are somewhat distinctive from AD and other neurodegenerative disorders [2, 43]. Here we found evidence of volumetric improvement in brain regions implicated in MS atrophy [40, 44], as well as AD signature atrophy regions (e.g., left inferior parietal, right banks of the superior temporal sulcus, left medial orbitofrontal, left superior temporal, right medial orbitofrontal cortex, and right frontal pole [45, 46]. In late MS and with predominance of the neurodegenerative phenotype, GM atrophy is more strictly connected to progression of disability than WM atrophy [4 , 48]. Our results show promise for iCR-based diets to target neurodegeneration in both MS and AD.
DBSI model uses a combination of anisotropic and isotropic diffusion tensors to model both the axonal myelin integrity and intra-fiber and interstitial inflammation, reflected by increased edema and tissue cellularity [26, 49]. Together with existing literature our results support an effect for iCR in reducing 1) vasogenic edema (reduced HF), 2) fiber free water (decreased AD and RD and increased FA), 3) inflammatory infiltrates (reduced RF), and 4) axonal injury and demyelination (reduced isotropic HF and increased FA), in midlife individuals with MS [18 , 51]. Neuroinflammation expressed as increased cellularity and microstructural changes in brain’s grey and white matter is another shared pathomechanism between MS and AD. While grey matter atrophy is a major biological substrate of cognitive decline in AD, axonal loss, demyelination, and neuroinflammation are now considered to be mechanistically fundamental to the AD pathology [52, 53]. Indeed, evidence of increase cellularity and disruption of WM integrity can be detected in both preclinical and early symptomatic phases of AD [53, 54]. Ultimately, in both MS and AD, prolonged neuroinflammation leads to WM atrophy with disease specific patterns that are discernible in late disease [55, 56]. Among WM tracts showing reduced inflammation with iCR in our study, cerebellar peduncles are known as common areas for T2/FLAIR abnormalities in MS [57, 58]. iCR was also able to reduce inflammation in form of vasogenic edema in the left optic tract of our MS patients. Intriguingly, retinal and optic pathway, often unequivocally affected by MS pathology [59, 60].
Limitations
Given the pilot nature of the study and the small sample size, individual changes in the studies biomarkers might be insufficient in reflecting the effects of iCR. Aiming to recruit 50 participants in each arm of the study we hope to achieve 80% power in studying the volumetric differences between the two groups as the main outcome of the study. Also, while we aim to study equivalent proportions of men and women in this study once complete, the current pilot data represents disproportionate number of men versus women. Similarly, participant’s age, MS subtype, years since diagnosis, and type of disease modifying therapy might be better matched once recruitment is complete in both groups. While we are not specifically designed or powered to investigate a potential sexual dimorphism or the effect of disease-specific traits on response to iCR diet, we understand that addressing these differences could be an interesting point of discussion and reveal trends that can be addressed in future studies. Caution should be exerted in implementing caloric restrictive diets in elderly population and those with existing metabolic or neurodegenerative condition or in middle aged adults at risk for malnutrition.
Conclusion
iCR was able to prevent brain volume loss in signature regions previously indicated in AD and MS, while mitigating neuroinflammation in WM tracts implicated in the pathology of MS and pre-clinical AD. CR-based diets have potential as anti-inflammatory and neuroprotective interventions in mid-life individuals.
Footnotes
ACKNOWLEDGMENTS
This research was supported by the grant number 1RF1AG072637-01 (CR). Additional support was provided by the Charles and Joanne Knight Alzheimer Disease Research Center Support Fund and the Barnes-Jewish Hospital Foundation, and the Radiological Society of North America Research Scholar Grant.
FUNDING
This work is supported by grant number 1RF1AG072637-01 from the National Institute on Aging.
CONFLICT OF INTEREST
Dr. Raji consults for Brainreader ApS, Icometrix, Neurevolution LLC, and AHNP Precision Health.
Dr. Raji is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review.
DATA AVAILABILITY
The data supporting the findings of this study are available upon request from the corresponding author.