
Abstract
Background:
Alcohol use disorders have been categorized as a ‘strongly modifiable’ risk factor for dementia.
Objective:
To investigate the cross-sectional association between alcohol consumption and cognition in older adults and if it is different across sexes or depends on amyloid-β (Aβ) accumulation in the brain.
Methods:
Cognitively unimpaired older adults (N = 4387) with objective and subjective cognitive assessments and amyloid positron emission tomography (PET) imaging were classified into four categories based on their average daily alcohol use. Multivariable linear regression was then used to test the main effects and interactions with sex and Aβ levels.
Results:
Individuals who reported no alcohol consumption had lower scores on the Preclinical Alzheimer Cognitive Composite (PACC) compared to those consuming one or two drinks/day. In sex-stratified analysis, the association between alcohol consumption and cognition was more prominent in females. Female participants who consumed two drinks/day had better performance on PACC and Cognitive Function Index (CFI) than those who reported no alcohol consumption. In an Aβ-stratified sample, the association between alcohol consumption and cognition was present only in the Aβ– subgroup. The interaction between Aβ status and alcohol consumption on cognition was not significant.
Conclusion:
Low or moderate consumption of alcohol was associated with better objective cognitive performance and better subjective report of daily functioning in cognitively unimpaired individuals. The association was present only in Aβ– individuals, suggesting that the pathophysiologic mechanism underlying the effect of alcohol on cognition is independent of Aβ pathology. Further investigation is required with larger samples consuming three or more drinks/day.
INTRODUCTION
Alcohol consumption is a potentially modifiable behavior and therefore there is a public health imperative to understand its effect on health outcomes. The complexity in understanding the relation between alcohol consumption and health outcomes arises from the possible protective effect of low to moderate alcohol consumption resulting in “J-shaped” or “inverse U-shaped” associations between quantity of alcohol use and mortality [1], cardiovascular disease [2], and cognition [3]. Excessive alcohol consumption has also been identified as one of the risk factors for Alzheimer’s disease and related dementias (ADRD) [4–7]. However, data on effects of low or moderate alcohol consumption on cognition is inconclusive. Some studies support the view that low or moderate alcohol consumption may reduce Alzheimer’s disease (AD) dementia risk [8–10]; however, these positive effects can be out-weighed by increased risk for other health conditions [11].
Alcohol use disorders have been categorized as a ‘strongly modifiable’ risk factor for dementia [12]. However, our understanding of the underlying pathophysiologic mechanisms for the observed association between alcohol consumption, cognitive decline, and AD is limited. Little information is available regarding the association between alcohol consumption and the in vivo AD biomarkers of amyloid-β (Aβ), tau, or neurodegeneration. MRI studies suggest that moderate alcohol consumption might have a protective effect against neurodegeneration and cerebrovascular disease [13, 14]. PET studies suggest that older adults with moderate lifetime alcohol intake have lower Aβ levels compared to those who do not drink [15]; however, these findings are not supported by postmortem neuropathological studies [16]. Understanding the relation between Aβ accumulation in brain and the effects of modifiable risk factors, like alcohol, on cognition is crucial to developing public health prevention strategies. In particular, understanding the physiological and neurological effects associated with low or moderated alcohol consumption is critical to tracking the progression of cognitive impairments or improvements in pre-clinical AD population. In addition, it is equally important to analyze these effects across key characteristics of the population, especially considering the sex-differences or other demographic factors.
In this study, we used the screening data from pre-randomization visits of the Anti-Amyloid Treatment in Asymptomatic Alzheimer’s Disease (A4 Study). The A4 Study is a global, randomized controlled trial investigating the effect of a monoclonal antibody on slowing cognitive decline targeting older adults in preclinical stages of AD. We investigate the effect of different alcohol consumption profiles on cognitive function using standardized and sensitive objective and subjective cognitive assessments from the A4 Study. We examined alcohol consumption as a continuous variable (self-reported daily consumption reported as ‘drinks per day’ (DPD): ranging from 0 to 30) as well as in groups of no- (0 DPD), low/moderate- (1 or 2 DPD), or high-alcohol consumption (≥3 DPD). While differences in alcohol consumption patterns and quantity among men and women are well established, the effect of sex on the relationship between alcohol consumption and cognition is less clear [17, 18]. Therefore, we also investigated the effects of alcohol consumption on cognition by sex groups. We hypothesized that low/moderate alcohol consumption will correlate with a better cognitive performance compared to that of no- or high-alcohol consumption. Furthermore, to improve our mechanistic understanding of this effect, we evaluated if there is a differential association between alcohol and cognition among those with elevated Aβ positive (Aβ+) and those with normal Aβ levels (Aβ–).
MATERIALS AND METHODS
Participants
We used data from participants in the A4 Study, which was conducted at 67 sites across the United States, Canada, Australia, and Japan [19] (https://clinicaltrials.gov/ct2/show/NCT02008357). Institutional review board approval was obtained at each site. All participants provided written informed consent before participation. The A4 and LEARN Studies are coordinated by Alzheimer’s Therapeutic Research Institute (ATRI) at the University of Southern California, and the data are made available through the Laboratory for Neuro Imaging at the University of Southern California [19]. A total of 6,763 individuals with normal cognition between age 65 and 85 years were initially screened for A4 Study enrollment. Participants with a Clinical Dementia Rating (CDR) global score of 0, Mini-Mental State Examination (MMSE) score of 25 to 30, and Logical Memory Delayed Recall test score of 6 to 18 were eligible for fluorine 18– labeled-florbetapir positron emission tomography (PET) imaging. A total of 4,486 participants underwent a PET scan [20]. For the purpose of this study, we used data from the participants who had an amyloid PET scan and answered the lifestyle questionnaire. Out of the 4486 participants who underwent PET scans, 54 people were excluded from the study due to incomplete datasets (Fig. 1).
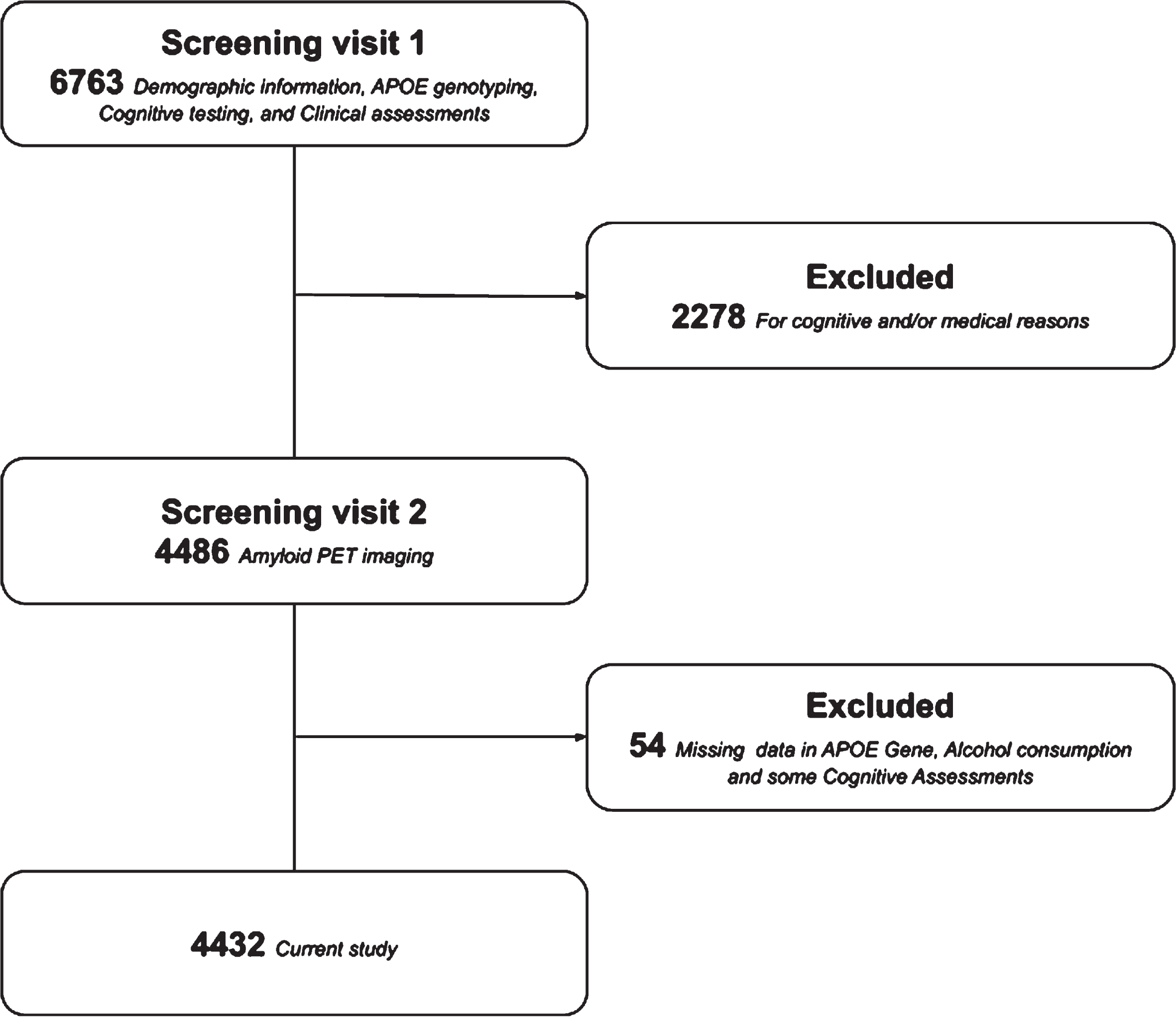
A4 study first 2 screening visits and current work.
Cognitive assessments
The Cognitive Function Index (CFI), a questionnaire that assesses change in cognition and daily functional abilities over the previous year [21] was separately completed by each of the participants and their respective study partner (score range: 0–15, with higher scores indicating worse reported cognitive function).
Objective assessment of participant’s cognition was completed using the Preclinical Alzheimer Cognitive Composite (PACC), a composite score calculated as the average of the sum of standardized scores on the following tests [20]: MMSE, a measure of global cognition (range, 0–30). Delayed Logical Memory (DLM), recall of a narrative story 15 minutes after initial recall (range, 0–25). Digit Symbol Substitution Test (DSST), a measure of executive function (maximum score, 91) [22]. Free and Cued Selective Reminding Test (FCSRT), a multi-trial word recall test. Scores includes the sum of free recall (FR) alone (range 0–48) and combined with total recall (TR), and the sum of FR and TR (TR96: range 0–96) [23].
Since the range and sensitivity of the MMSE and logical memory are limited in this patient population, we focused on FSCRT and DSST scores as the main objective outcomes [24].
Amyloid PET imaging
Amyloid PET imaging was done using 18F-florbetapir data, acquired 50–70 min post injection. Images were realigned and averaged, and then spatially aligned to a standard space template. 18F-florbetapir, sampled in a global neocortical region for Aβ, was expressed as a standardized uptake value ratio (SUVR) with a cerebellar reference region. Aβ positivity was defined as participants with 18F-florbetapir PET SUVR >1.15 [25].
Lifestyle variables
The quantity of individuals’ alcohol consumption was assessed from their response to the question “average number of alcoholic drinks consumed per day” in a brief self-report questionnaire about their current lifestyle. This questionnaire was given in the screening visit of the A4 study, and it also included several other questions such as typical number of hours of sleep per night, amount of aerobic physical activity, and caffeinated drinks per day. Previous studies suggest that that the relationship between alcohol consumption and cognition is non-linear [8, 26]. Specifically, moderate alcohol consumption has been found to be beneficial when compared with no alcohol consumption or prominent levels of alcohol consumption [8, 9]. Based on these findings and considering generally different guidelines on recommended amounts of alcohol for females and males [27], we categorized daily alcohol consumption (DAC) into four groups of 0 (50% of the total participants included in the study, N = 4432), 1 (32% of N), 2 (12% of N), and 3 or more (≥3, 6% of N) alcoholic drinks per day.
Statistical analyses
Demographic characteristics of the DAC groups were compared using analysis of variance for continuous variables and χ2 tests for categorical variables, with Cramer’s V measure for effect size. Associations between alcohol consumption and cognitive scores were assessed using linear regression (the assumptions of linear regression were verified to hold for the objective measures). The outcomes of cognitive scores used in the regression models included the CFI score of the participants, the composite score PACC as well as the individual scores from two of the four tests that comprise PACC (FSCRT and DSST). Analyses were repeated using a 4-factor categorical variable for DAC in linear regressions: 0, 1, 2, and ≥3 alcoholic DPD, with post-hoc contrasts examined. Given that most cognitively normal older individuals are at the upper score limit of FSCRT total recall score, even small decrements in cueing are associated with early changes related to AD. Therefore, we used logistic regressions to identify association between DAC and the maximum FCSRT total recall score (48 versus <48). Age, sex, and years of education were included in models as covariates. No multiple comparisons correction was performed. We considered 2-sided p < 0.05 to be statistically significant. All statistical analyses were performed using Python (3.7.12).
RESULTS
Sample characteristics
The 4,432 participants included in the study had a mean (SD) age of 71.28 (4.67) years, 16.58 (2.84) years of education, and 2,631 (59%) were women (Table 1). Men had higher DAC in comparison with women (χ2 = 108.86, p < 0.001, Cramer’s V = 0.157). Participants with higher education reported higher daily consumption of alcohol (p < 0.001). White participants consumed more alcohol in comparison with all other races (χ2 = 80.70, p < 0.001, Cramer’s V = 0.08). There was no relationship between a participant’s age or APOE4 status and DAC.
Alcohol consumption by demographic characteristics
Other in Race / Ethnicity includes participants from races: American Indian or Alaskan Native, Asian, Native Hawaiian or Other Pacific Islander or where no data was available.
Alcohol consumption and cognition in whole population
Linear regression models indicated self-reported DAC is associated with the PACC scores (β [SE] = 0.07 [0.03]; p = 0.015), scores in FR-FCSRT (β [SE] = 0.16[0.07]; p = 0.019), and DSST (β [SE] = 0.22 [0.11], p = 0.041) (Table 2).
Alcohol consumption and cognition
PACC, Preclinical Alzheimer Cognitive Composite (a composite score calculated as the average of the sum of standardized scores from other assessments); DSST, Digit Symbol Substitution Test; FCSRT, Free (FR) and Cued (CR) Selective Reminding Test; FCSRT96, 2*FR + CR; MMSE, Mini-Mental State Examination; CFI, Cognitive Function Index (lower scores are better). All the values except ‘count’ indicate mean (SD). Linear regression models indicate that daily alcohol consumption is associated with the participants’ PACC scores, and scores in FR-FCSRT and DSST (p-values <0.05 are highlighted in bold).
PACC scores were found to be significantly worse in the participants who reported consuming no alcohol in comparison with the participants who reported consuming 1 drink/day (β [SE] = 0.19[0.08]; p = 0.017) or 2 drinks/day (β [SE] = 0.22[0.11]; p = 0.050) (Fig. 2A; Table 3). Participants who reported consuming no alcohol performed significantly worse on DSST in comparison with participants who reported consuming 1 drink/day (β [SE] = 0.78[0.29]; p = 0.007) or 2 drinks/day (β [SE] = 0.95[0.41]; p = 0.021) (Fig. 2B; Table 3). Participants who consumed 2 drinks/day had higher scores on the FR-FSCRT in comparison with those who reported no alcohol consumption (β [SE] = 0.56 [0.25]; p = 0.025) (Fig. 2C; Table 3). No other significant differences between alcohol consumption groups in objective cognitive scores were observed.
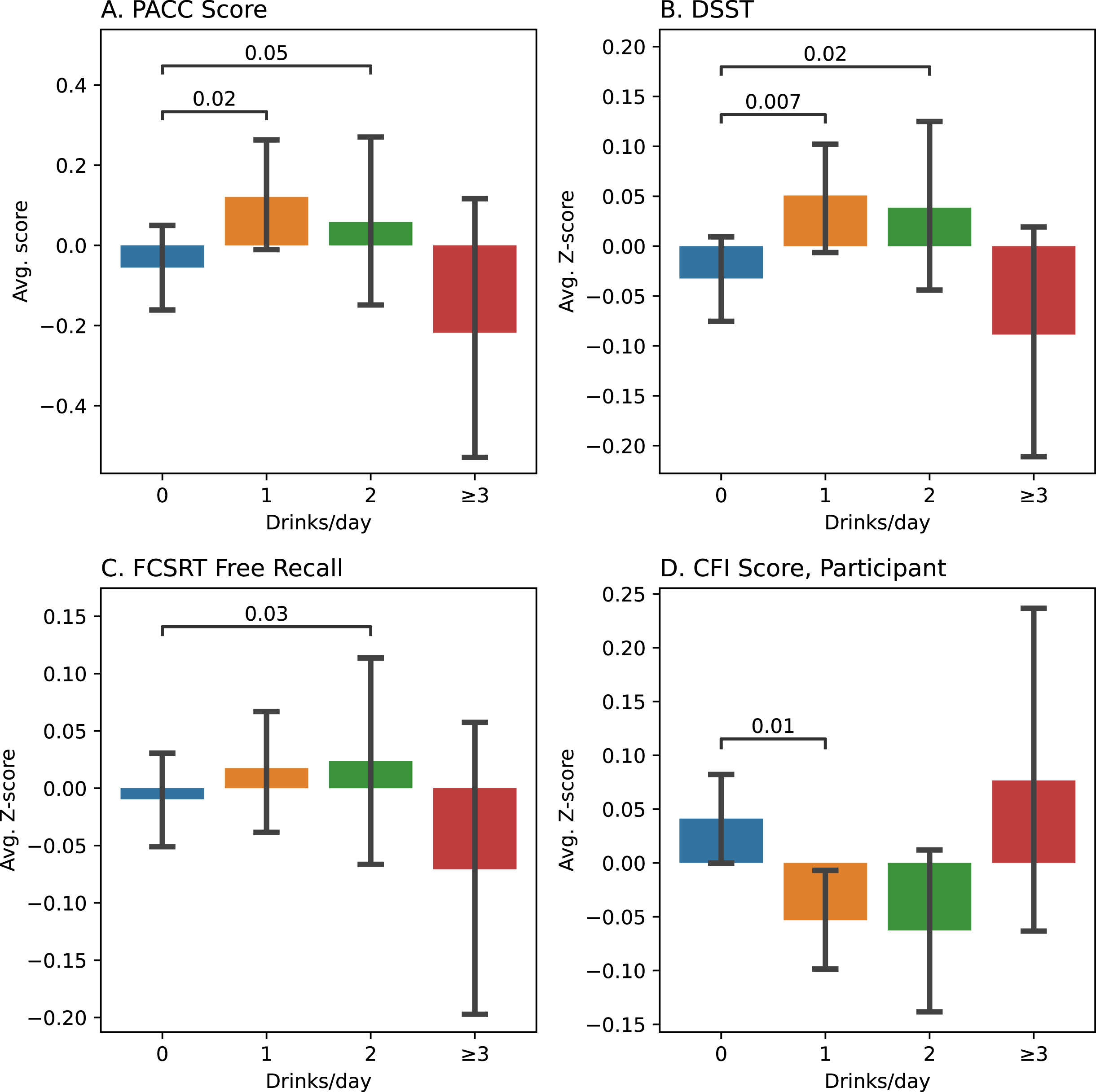
Cognitive test scores across Alcohol consumption groups among all Participants. PACC, Preclinical Alzheimer Cognitive Composite (a composite score calculated as the average of the sum of standardized scores from other assessments); DSST, Digit Symbol Substitution Test; FCSRT, Free and Cued Selective Reminding Test; CFI, Cognitive Function Index (lower scores are better). Bars indicate 95% CI, Between-group differences when significant are marked with p-values. Z-score: Normalized score across the whole population.
Cognition across Alcohol consumption groups among all participants
PACC, Preclinical Alzheimer Cognitive Composite (a composite score calculated as the average of the sum of standardized scores from other assessments); DSST, Digit Symbol Substitution Test; FCSRT, Free (FR) and Cued (CR) Selective Reminding Test; CFI, Cognitive Function Index (lower scores are better). p-values <0.05 are highlighted in bold.
Subjective report of cognitive impairment (SCI), measured by the CFI questionnaire, also differed based on DAC. Participants who consumed 1 alcoholic drink/day had lower SCI compared to those who consumed no alcohol (β [SE] = –0.15(0.06); p = 0.012) (Fig. 2D; Table 3). There were no differences in SCI as reported by the study partners across the alcohol consumption groups. Group differences in cognitive scores across DAC groups were further assessed using a separate ANCOVA analysis with pairwise comparisons (Supplementary Table 1).
Effect of sex on the association between alcohol consumption and cognition
In the whole sample, females performed better than men across subjective and objective cognitive measures (β [SE], p-value - PACC: 1.26(0.07), <0.001; DSST: 3.14(0.26), <0.001; FR-FCRST: 2.95(0.16), <0.001; TR-FCRST: 0.24(0.03), <0.001; Fig. 3). In regression models that included a sex-by-DAC interaction term in addition to the other covariates, only the interaction term for FR-FCSRT was significant (p = 0.032, Supplementary Table 2). However, based on our prior hypothesis and given the large sample size, we repeated the analysis for the sex-stratified samples and conducted post-hoc analyses to study within-group differences across all alcohol consumption groups for both thesexes.
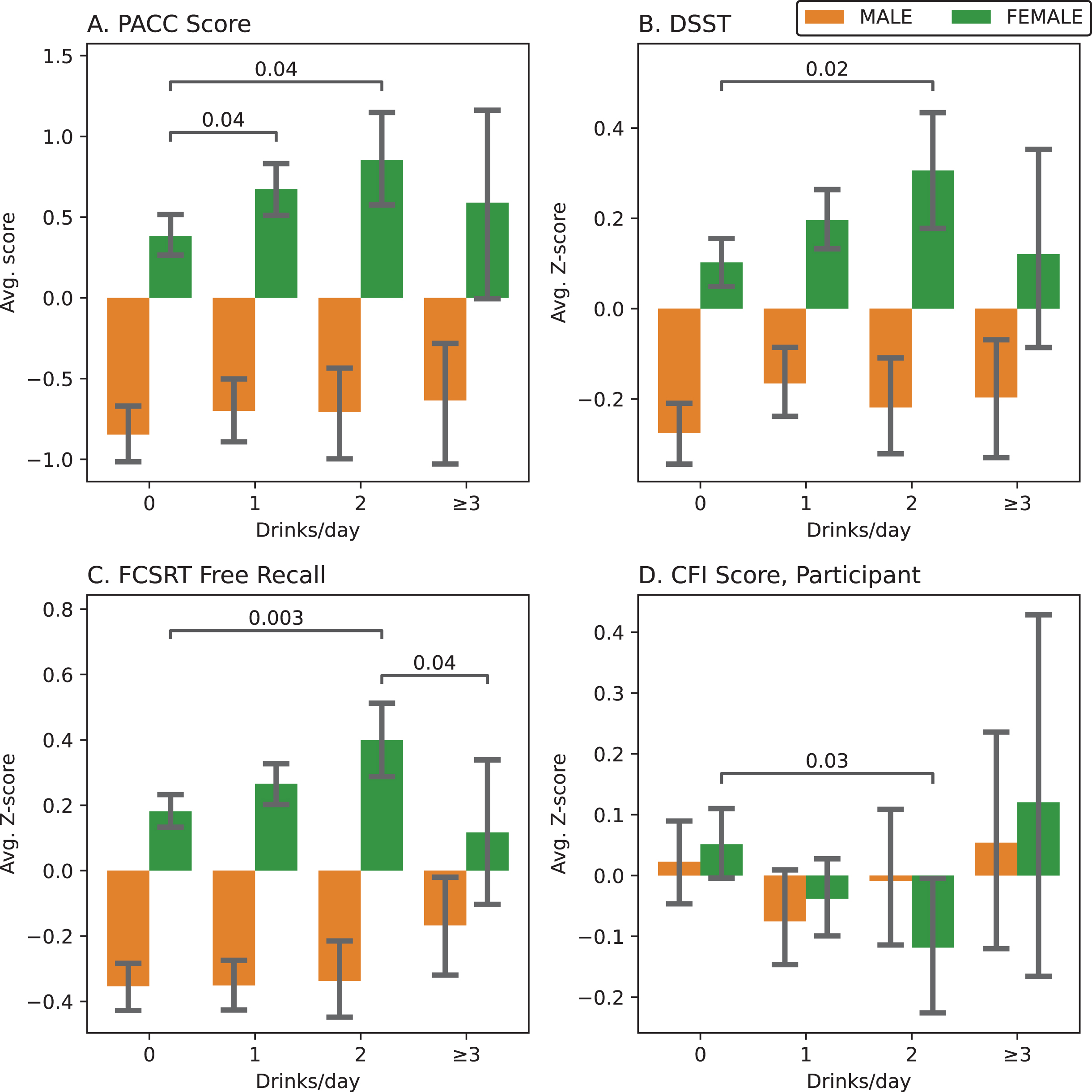
Cognitive test scores across Alcohol consumption groups in men (left) and women (right). PACC, Preclinical Alzheimer Cognitive Composite (a composite score calculated as the average of the sum of standardized scores from other assessments, population mean[SD] – Female: 0.53[2.46], Male: –0.76[2.44]); DSST, Digit Symbol Substitution Test; FCSRT, Free and Cued Selective Reminding Test; CFI, Cognitive Function Index (lower scores are better). Bars indicate 95% CI, Between-group differences when significant are marked with p-values for Female (green) participants. Z-score: Normalized score across the whole population, before stratifying the data.
PACC scores of female participants who reported consuming no alcohol were significantly worse than those consuming 1 drink/day (β [SE] = 0.21[0.10]; p = 0.038) or 2 drinks/day (β [SE] = 0.32[0.16]; p = 0.043) (Fig. 3A; Table 4). Females who reported consuming no alcohol performed significantly worse on the DSST than those who reported consuming 2 drinks per day (β [SE] = 1.36[0.59]; p = 0.022) (Fig. 3B; Table 4). Additionally, the FR-FCRST scores of females who consumed 2 drinks per day were significantly higher than those who consumed either 3 or more drinks per day (β [SE] = –1.42[0.67]; p = 0.036) as well as than those who consumed no alcohol at all (0 versus 2: β [SE] = 1.02[0.34]; p = 0.003) (Fig. 3C; Table 4). Women who consumed 2 alcoholic drinks/day had lower CFI scores (better subjective cognitive function) compared to those who consumed no alcohol (β [SE] = –0.27[0.12]; p = 0.026) (Fig. 3D; Table 4). Male participants reporting no alcohol consumption performed better than those reporting 1 DPD on the DSST (β [SE] = 1.07[0.45]; p = 0.017) and better than those who consumed 3 or more drinks per day on the FR-FCRST (β [SE] = 1.09(0.48); p = 0.022) (Fig. 3; Table 4).
Cognition across Alcohol consumption groups: Participants stratified by Sex
PACC, Preclinical Alzheimer Cognitive Composite (a composite score calculated as the average of the sum of standardized scores from other assessments); DSST, Digit Symbol Substitution Test; FCSRT, Free (FR) and Cued (CR) Selective Reminding Test; CFI, Cognitive Function Index (lower scores are better). p-values <0.05 are highlighted in bold.
Effect of Aβ status on the association between alcohol consumption and cognition
When an interaction term for Aβ status and DAC were added to regression models, no significant interaction was observed. Again, based on our prior hypothesis, we stratified the sample into Aβ– and Aβ+ subgroups based on the levels of amyloid PET SUVR (see methods for details) and repeated the analysis. Within the Aβ– subgroup, a few significant differences across the alcohol consumption groups were observed. Specifically, participants who reported consuming no alcohol performed significantly worse in comparison with those who reported consuming 1 drink/day on the PACC (β [SE] = 0.28[0.09]; p = 0.003) (Fig. 4A; Table 5, the DSST (β [SE] = 0.84 [0.34]; p = 0.014) (Fig. 4B; Table 5) and the FR-FCRST (β [SE] = 0.53[0.21]; P = 0.012) (Fig. 4C; Table 5). Among Aβ– subgroup, participants who consumed 1 alcoholic drink/day had lower SCI compared to those who consumed no alcohol (β [SE] = –0.18(0.07); p = 0.009) (Fig. 4D; Table 5). There were no significant differences in cognitive scores across alcohol consumption groups in Aβ+ subgroup (Table 5). In a separate preliminary analysis using similar regression models, the age-by-sex and age-by-Aβ interaction terms were found to be significant for PACC and DSST outcomes (Supplementary Table 2).
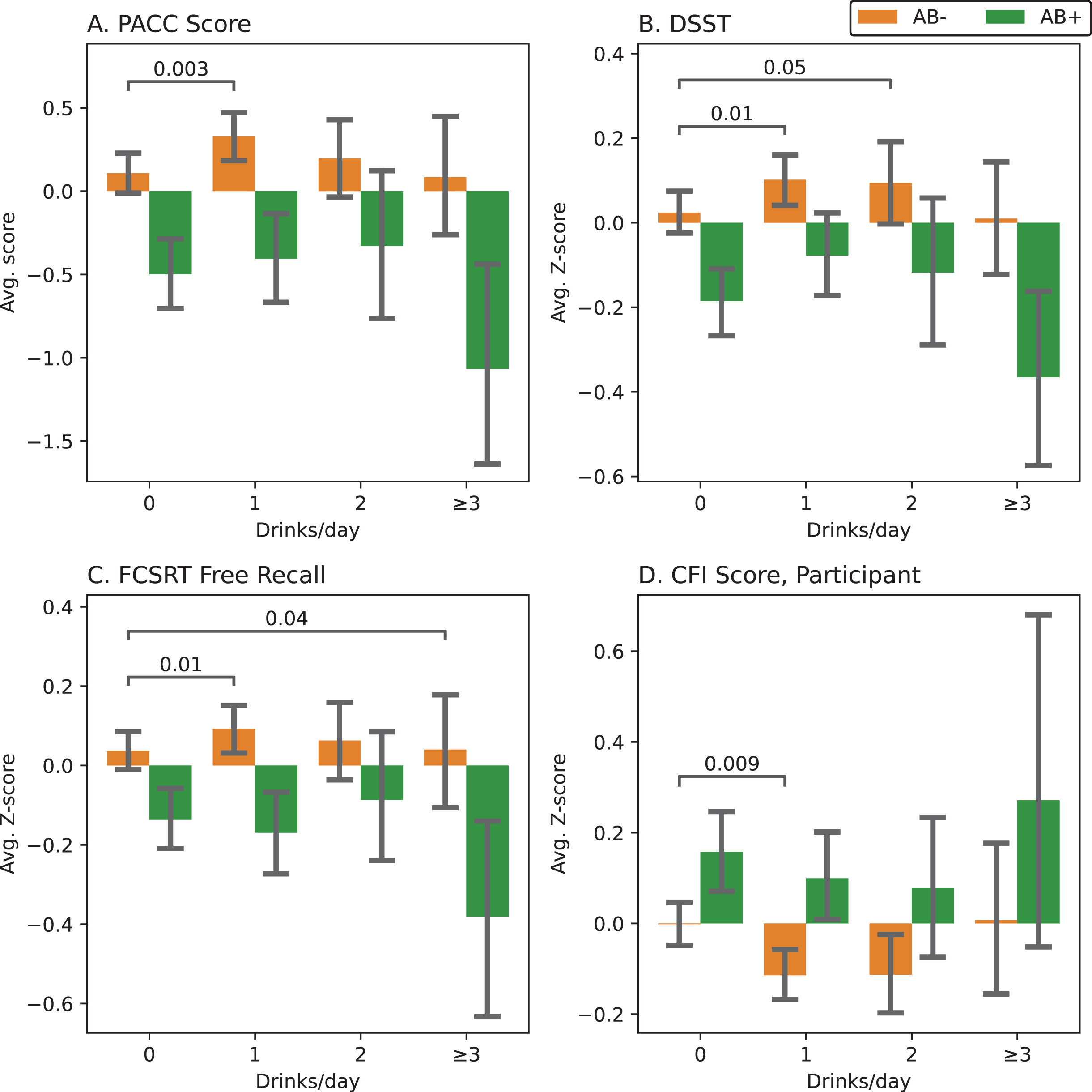
Cognitive test scores across Alcohol consumption groups in Aβ+ (right) versus Aβ– (left) individuals. PACC, Preclinical Alzheimer Cognitive Composite (a composite score calculated as the average of the sum of standardized scores from other assessments, population mean[SD] – Aβ– : 0.19[2.46], Aβ+: –0.47[2.65]); DSST, Digit Symbol Substitution Test; FCSRT, Free and Cued Selective Reminding Test; CFI, Cognitive Function Index (lower scores are better). Bars indicate 95% CI, Between-group differences when significant are marked with P-values for Aβ– individuals (orange) participants. A Composite PET SUVR of 1.15 is used as a cut-off for elevated Aβ (Aβ+). Z-score: Normalized score across the whole population, before stratifying the data.
Cognition in Population groups across Alcohol consumption groups: Stratified by elevated Aβ levels (Aβ+ or Aβ–)
PACC, Preclinical Alzheimer Cognitive Composite (a composite score calculated as the average of the sum of standardized scores from other assessments); DSST, Digit Symbol Substitution Test; FCSRT, Free (FR) and Cued (CR) Selective Reminding Test; CFI, Cognitive Function Index (lower scores are better). p-values <0.05 are highlighted in bold. Aβ+/ Aβ–, Elevated/Not-elevated amyloid-beta levels as measured by PET-SUVR (Elevated: Composite PET-SUVR ≥1.15).
DISCUSSION
In this study, we observed an association between self-reported daily alcohol consumption (DAC) and cognitive performance in cognitively unimpaired older adults as measured by different objective and subjective assessments. Overall, our results indicate that low or moderate alcohol consumption as opposed to abstinence was associated with better scores in PACC, DSST, and FR-FCSRT and lower scores on CFI (better subjective cognitive function). In a sex-stratified sample of females but not in that of males, the results indicated that low or moderate alcohol consumption, as opposed to abstinence, was associated with better scores on the PACC, DSST, and FR-FCSRT (also in comparison with excessive consumption) and lower scores on CFI. Similar results were found in the Aβ– subgroup when the population was stratified by elevated Aβ status, but not in the Aβ+ subgroup.
Consumption of large amount of alcohol is known to have negative impact on cognition and is associated with increased risk of cognitive decline and dementia [28, 29]. However, alcohol consumption in smaller amounts may have protective effect [8–10]. Our results are largely in agreement with previous studies, indicating an inverted U-shaped pattern in the associations between self-reported alcohol consumption and cognitive function. Participants with low or moderate alcohol consumption had better cognitive performance based on both subjective and objective measures. Participants who reported no alcohol consumption performed generally better than those who reported excessive consumption. The positive influence of low to moderate drinking on cognition and health, has been attributed to stress relief, mood relaxation, and decreased risk of cardiovascular disease and strokes [30].
Alcohol consumption rates differ between men and women [31]. Furthermore, effects of alcohol on brain and cognition are different amongst the sexes [32]. It was previously reported that among the subjects diagnosed with substance-dependence that included alcohol-dependence, women progressed more rapidly towards requiring the substance-abuse treatment than men and reported more psychiatric problems [33] as measured by an Addiction Severity Index prior to the treatment. Although there were no significant differences found across sexes in alcohol severity at treatment entry, women reported significantly higher psychiatric problems highlighting the difference in psychopathology across the sexes. Brain aging, which represents a decrement in the structural brain health (measured using structural MRI), was reported to be accelerated in females with a family history of AD compared to their male counterparts [34]. Such views have been challenged, however, by reports showing little evidence for sex-differences in the course of alcohol dependence [35] and by studies reporting less accelerated brain aging process in females than males under different circumstances [36–38]. In our sample, men consumed more alcohol than women and women had better overall performance on most cognitive tests. Our results also indicate a sex-by-DAC interaction for FR-FCSRT suggesting a differential effect of alcohol consumption on cognition in women than men. In sex-stratified samples, the significant associations between cognition and DAC were mostly observed in the female participants. Lack of significant findings in male subgroup might suggest sex-specific effects of alcohol on cognition [18, 39–41]. It is possible that such differences in sexes in neuro-psychological assessments could be due to a greater susceptibility to abnormalities in brain structure and volume in women than men [42–44].
Despite known long-term effects of alcohol consumption on cognition, the underlying brain pathophysiology that moderates alcohol effects is not clear. Prior studies highlight mixed effects of alcohol on the structural brain health involving white matter [45], cortical thickness [46], and hippocampal volume [46, 47] as potential underlying substrates moderating the effect of alcohol on cognition. In particular, it was shown in a large population-based cohort study [48] that even low alcohol consumption (7–14 units weekly) was associated with lower total grey matter volumes. These results highlight an overall negative association between alcohol consumption and total grey matter volume as opposed to the general view of “inverse U-shaped” associations between alcohol consumption and brain structure. A few studies also reported the relation between alcohol consumption and Aβ accumulation in the brain. In a study that assessed the relation between cerebral Aβ postmortem and alcohol consumption, especially using alcohol types, beer consumption was associated with lower Aβ aggregation [49]. Another study suggests that alcohol consumption adds to the cognitive burden seen in dementia by either increasing or sustaining Aβ aggregation via increased levels of neuroinflammation [50], suggesting lower alcohol consumption leads to lower Aβ aggregation. Cognitively unimpaired individuals with evidence of elevated biomarkers like Aβ have demonstrated substantial decline in both objective [51–53] and subjective assessments [54]. In our study, Aβ status did not explain the association between DAC and cognition (based on Aβ-by-DAC interaction term), however the association between cognition and DAC differed in samples stratified on Aβ status. Among the Aβ– participants, low- or moderate-alcohol consumption groups were associated with better scores on several objective and subjective assessments compared to abstinence, following the general inverted U-shaped pattern (U-shaped for CFI) as seen in the whole population. The findings may indicate that the mechanisms underlying the effect of alcohol on cognition be independent of Aβ pathology. Further investigations using longitudinal biomarker studies are required to elucidate the underlying pathophysiology.
There are several limitations to this study. The alcohol consumption data was based on personal reports and thus subject to recall bias. Furthermore, the type and exact amount of alcohol consumption was not assessed; participants only reported “number of average drinks per day”. To accurately evaluate effects of varying levels of alcohol consumption, ideally, the consumption data should be standardized in terms of volumes specific to commonly consumed types of alcohol (for e.g., 1 US drink = 12 oz. of beer = 5 oz of wine = 1.5 oz of hard liquor [55–57]). Moreover, the reports of no alcohol consumption are indistinguishable between lifetime abstainers and those who reported no consumption at the time of study, which could be an important factor to better understand the implications of no or low alcohol consumption. The majority of the A4 study participants were white and non-Hispanic, therefore the results are limited to these population demographics. Also, lack of significant findings within the male subgroup and the Aβ+ subgroup could be related to the imbalance in sample sizes across alcohol consumption groups (DAC, no: 36% men; excessive: 66% men) as well as the size of whole sample (Aβ– : ∼72%). Although the data has been analyzed in stratified subsets by sex and elevated Aβ levels separately, more complex interactions need to be thoroughly explored especially among factors like sex, genetic predisposition, family history of disease, and accumulation of pathological biomarkers. Finally, due to the cross-sectional nature of the study design, causal inferences cannot bemade.
In conclusion, the findings from this study provide support for the notions that low or moderate alcohol consumption is associated with better cognition in older adults. While this study did not find an optimal level of alcohol consumption corresponding to better cognitive function specific to each sex, it suggests that females and males might be differently vulnerable to the effects of alcohol consumption on brain structure and function. To understand the precise implications of alcohol consumption on cognitive health and disentangling the underlying pathophysiology, longitudinal studies are needed to account for the relationship of alcohol metabolism to sex, genetics and brain pathology.
Footnotes
ACKNOWLEDGMENTS
The A4 Study is a secondary prevention trial in preclinical Alzheimer’s disease, aiming to slow cognitive decline associated with brain amyloid accumulation in clinically normal older individuals. The A4 Study is funded by a public-private-philanthropic partnership, including funding from the National Institutes of Health-National Institute on Aging, Eli Lilly and Company, Alzheimer’s Association, Accelerating Medicines Partnership, GHR Foundation, an anonymous foundation and additional private donors, with in-kind support from Avid and Cogstate. The companion observational Longitudinal Evaluation of Amyloid Risk and Neurodegeneration (LEARN) Study is funded by the Alzheimer’s Association and GHR Foundation. The A4 and LEARN Studies are led by Dr. Reisa Sperling at Brigham and Women’s Hospital, Harvard Medical School and Dr. Paul Aisen at the Alzheimer’s Therapeutic Research Institute (ATRI), University of Southern California. The A4 and LEARN Studies are coordinated by ATRI at the University of Southern California, and the data are made available through the Laboratory for Neuro Imaging at the University of Southern California. The’participants screening for the A4 Study provided permission to share their de-identified data in order to advance the quest to find a successful treatment for Alzheimer’s disease. We would like to acknowledge the dedication of all the participants, the site personnel, and all the partnership team members who continue to make the A4 and LEARN Studies po’sible. The complete A4 Study Team list is available on: a4study.org/a4-study-team.
FUNDING
Authors of this study were supported in part by grants from the National Institute of Health (NIA K23 AG063993, A.E.; 2PO1 AG003949, R.B.L); the Alzheimer’s Association (2019-AACSF-641329; A.E.); Cure Alzheimer Fund (A.E. & R.B.L.), the Leonard and Sylvia Marx Foundation (R.B.L.). None of the sponsors had any role in the design, methods, data acquisition, analysis, and preparation of the manuscript.
CONFLICT OF INTEREST
A.E is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review.
DATA AVAILABILITY
The data supporting the analyses of this study are available upon request from the website of Laboratory for Neuro Imaging at the University of Southern California at https://ida.loni.usc.edu/home/projectPage.jsp?project=A4 (![]() ).
).