
Abstract
Background:
Age-related cognitive decline is a chronic, progressive process that requires active clinical management as cognitive status changes. Computerized cognitive training (CCT) provides cognitive exercises targeting specific cognitive domains delivered by computer or tablet. Meanwhile, CCT can be used to regularly monitor the cognitive status of patients, but it is not clear whether CCT can reliably assess cognitive ability or be used to diagnose different stages of cognitive impairment.
Objective:
To investigate whether CCT can accurately monitor the cognitive status of patients with cognitive impairment as well as distinguish patients with dementia from patients with mild cognitive impairment (MCI).
Method:
We included 116 patients (42 dementia and 74 MCI) in final analysis. Cognitive ability was assessed by averaging the patient performance on the CCT to determine the Cognitive Index. The validity of the Cognitive Index was evaluated by its correlation with neuropsychological tests, and internal consistency was measured to assess the reliability. Additionally, we determined the diagnostic ability of the Cognitive Index to detect dementia using receiver operating characteristic (ROC) analysis.
Results:
The Cognitive Index was highly correlated with the Montreal Cognitive Assessment (r = 0.812) and the Mini-Mental State Examination (r = 0.694), indicating good convergent validity, and the Cronbach’s alpha coefficient was 0.936, indicating excellent internal consistency. The area under the ROC curve, sensitivity, and specificity of the Cognitive Index to diagnose dementia were 0.943, 83.3%, and 91.9%, respectively.
Conclusions:
CCT can be used to assess cognitive status and detect dementia in patients with cognitive impairment.
Keywords
INTRODUCTION
Age-related dementia is a chronic, progressive neurodegenerative syndrome [1]. During the early stages of dementia, patients suffer cognitive impairment but still maintain the ability to independently manage activities of daily living, and these patients are given a diagnosis of mild cognitive impairment (MCI) [2]. The cognitive status of patients with dementia can be classified into different stages, and it takes from several up to a dozen of years from the first signs of decline for patients to develop severe dementia [3]. Because medical treatments and other healthcare for patients with cognitive impairment are adjusted over the course of progressive disease, validating cognitive status and longitudinal cognition monitoring can greatly assist with disease management [4]. Also, because the rate of decline of cognitive function of patients with MCI can vary substantially, longitudinal monitoring of cognitive status in patients with MCI could have prognostic implications as well as help physicians tailor clinical interventions [5].
Digital technology-based cognitive assessments have several advantages for longitudinal cognition monitoring. Digital technology-based cognitive assessments are assessments presented in digital formats such as electronic version of traditional cognitive assessments [e.g., Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA)], computerized game-based assessments and virtual reality (VR)-based cognitive assessments. The paper-based cognitive assessments, such as the MMSE [6] or MoCA [7] are time- and medical resource-intensive as well as influenced by assessor bias [8, 9]. In contrast, digital technology-based cognitive assessments which are delivered by computer, tablet, or VR devices can partially overcome the difficulties met by paper-based assessments [9] and have the potential to be more convenient and cost-effective for longitudinal cognition monitoring [10]. Recent studies have shown the validity and reliability of computerized game-based cognitive assessments on healthy populations and patients with cognitive impairment. Wang et al. developed a new game-based cognitive assessment tool to assess cognitive status and enable early screening of patients with degenerative dementia and showed it had good diagnostic performance, with sensitivity and specificity of 85.1% and 91.5%, respectively [11]. Vyshedskiy et al. developed the Boston Cognitive Assessment, an online, self-administered test for longitudinal tracking of cognitive performance, which was shown to be without significant practice effects [12].
In addition to computer-based cognitive assessment tools, computerized cognitive training (CCT) is a digital health application designed to improve cognitive function. CCT is derived from traditional cognitive training tasks which are designed to target specific cognitive functions, such as attention, memory, thinking, and executive functions [13]. CCT involves the deployment of structured cognitive training tasks on computers or mobile electronic devices through the utilization of computer technology. By leveraging advancements in computer and tablet technology, CCT offers a platform for delivering cognitive training programs in a digital format [14, 15]. These programs typically consist of a series of interactive exercises and tasks which are designed based on psychological paradigms and require users to engage in various cognitive processes. Through repeated practice and feedback, CCT aims to enhance cognitive performance by strengthening neural connections, improving information processing, and promoting neuroplasticity [16, 17]. CCT has been proved efficient in improving cognitive abilities in both healthy old adults and patients with cognitive impairment [18–20].
CCT has the potential to make cognition monitoring more accessible by using home-based, online exercises designed to improve cognition and simultaneously provide longitudinal feedback on cognitive function [21]. As a monitoring strategy, CCT may even have important benefits versus traditional cognitive tests because it becomes feasible to average larger datasets over time and it also reduces random variations [22]. VR-based cognitive training has been shown to efficiently screen for MCI, and emerging data also suggest it may be a promising tool for longitudinal cognition monitoring [22, 23]. However, so far, studies investigating the utility of CCT and VR-based cognitive training for cognitive monitoring have been pilot studies with small sample sizes or have lacked validation of results with established neuropsychological assessment scales. Moreover, only a few of these studies assessed cognitive function in patients with dementia. Thus, additional studies are needed to determine whether CCT is a robust tool for cognition assessment.
In this study, we assessed the validity and reliability of a CCT program on cognitive assessment using one-week longitudinal performance of CCT. The CCT program was modified from a reported CCT program which was proven efficient at improving cognitive function in patients with MCI [18]. We also evaluated the ability of this CCT program to identify patients with dementia. The self-adapted CCT program contains 15 cognitive training tasks targeting five cognitive domains, and patient performance on each domain was averaged to generate a Cognitive Index. Our results suggest that CCT may be a useful tool to assess cognitive status and detect dementia in patients with cognitive impairment.
METHODS
CCT content
The training tasks included in the CCT targeted five cognitive domains: thinking, perception, attention, memory, and executive function. Every task was designed based on one or several classical cognitive training paradigms and these paradigms included pursuit-tracking task, continuous performance test, size-matching task, Corsi block-tapping task, visual search task, delayed match-to-sample test, face–name task, Stroop task, mental arithmetic task, flanker task, and spatial monitoring task (Supplementary Material). Each CCT training task was designed with several difficulty levels and cognitive training tasks targeting the same cognitive domain were designed to have equivalent difficulty at the same level to ensure the results of the cognitive assessment were consistent among different tasks.
Study population and study design
Participants were consecutively recruited from patients with cognitive impairment registered in the CCT program in 2021. Patient diagnosis was confirmed by neurologists based on symptoms, physical and neuropsychological examinations, and laboratory tests. Cognitive status was classified as MCI or dementia. The criteria for diagnosis with MCI were derived from the Petersen criteria: 1) cognitive complaints, 2) MoCA score between 18–26, 3) Basic Activity of Daily Living (BADL) [24] score >60, 4) without diagnosis of dementia. The MMSE and Clinical Dementia Rating Scale (CDR) [25] were used as objective assessments to diagnose dementia. MMSE scales were adjusted by educational level: ≥9 years, MMSE <24; <9 years, MMSE <20; no education, <17. The inclusion criteria were as follows: age >40 years; completed CCT tasks covering five cognitive domains within the first week; underwent neuropsychological assessments (MMSE and MoCA) within the first week. The exclusion criteria were unknown educational level or unknown age. The study protocol (NO. 2023-027) has been approved by the ethics committee of Xuanwu Hospital.
Demographic characteristics of study patients are provided in Table 1. We finally included 116 Chinese patients (42 patients with dementia and 74 patients with MCI). Patients in the MCI group had a mean age of 66.3±10.1 years (range from 43 to 90 years) and 60.8% of the patients were male. In the dementia group, the mean age of patients was 66.5±9.3 years (from 47 years to 87 years) and 64.3% were male. The average number of years of education was 12.5±3.6 and 10.7±3.7 in the MCI and dementia groups, respectively. Patients with dementia were classified into Alzheimer’s disease (AD), vascular dementia (VaD), and dementia with Lewy body (DLB) (AD, 31; VaD, 8; DLB, 3). The stage of dementia was also summarized in Table 1.
Patient demographics
SD, standard deviation; AD, Alzheimer’s disease; VaD, vascular dementia; DLB, dementia with Lewy body.
Administration of the CCT
Patients or their guardians voluntarily chose to undertake CCT at home on a tablet or computer. It was recommended that patients complete at least 20 min of the CCT per session and complete 3 sessions per week. Patients were informed that the difficulty of training tasks would be adjusted according to their performance. All cognitive training tasks for all five domains began at the lowest level of difficulty and subsequent tasks were tailored according to scores on the previous tasks. The training scores for each task were converted into normative scores based on the percentile rank in the population, and patient ability for each cognitive domain was calculated by averaging the scores of all tasks within a specific cognitive domain. Notably, when tasks within the same cognitive domain were completed on the same day, their scores were averaged to obtain the domain score for that day. However, if tasks within the same cognitive domain were performed on different days, the domain score was recalculated, overriding any previously assigned value. The Cognitive Index was calculated by averaging the scores for each cognitive domain (Fig. 1) and the Cognitive Index was updated when the patient finish taking a training task. The cognitive status within a week were assessed by the Cognitive Index updated on the last day in a week.
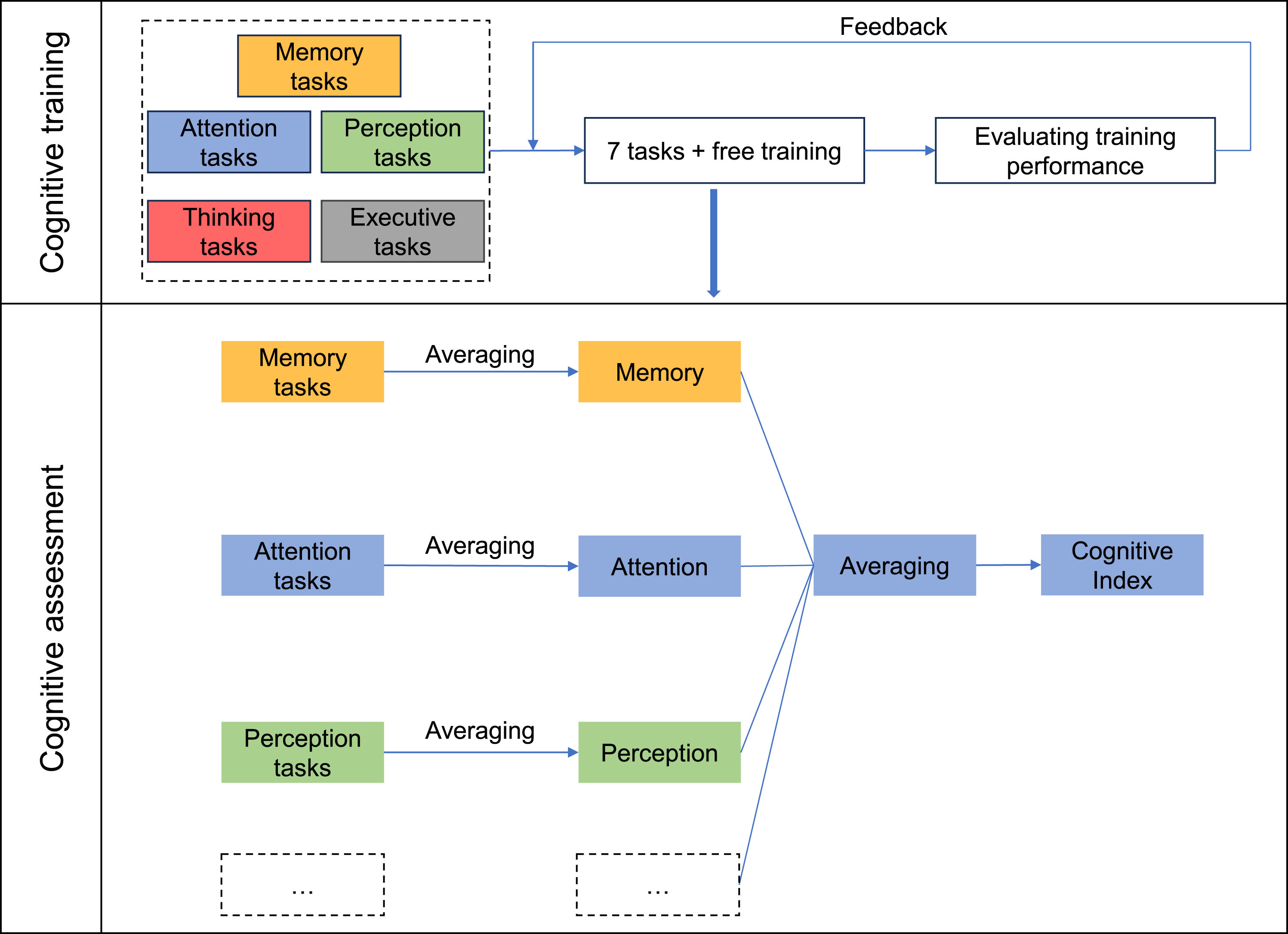
Diagram of cognitive assessment.
Neuropsychological assessment
Neuropsychological assessment was performed by the neurologists within the first week of the study using the MMSE and MoCA after patients had completed the initial required CCT tasks. The MMSE and MoCA scales were adjusted according to educational level.
Statistical methods
The Shapiro–Wilk test was used to examine the normal distribution of the Cognitive Index and the scores of neuropsychological assessments. Neither the Cognitive Index nor the neuropsychological assessment scores met the normality assumption with p < 0.05. Differences between groups were assessed using either independent samples t-test, Wilcoxon test, or Chi-Square test. We used Spearman’s correlation analysis to study the convergent validity of the CCT by analyzing the correlation between the Cognitive Index and neuropsychological assessment scores. Correlations between Cognitive Index and age and education level were also analyzed using Spearman’s correlation analysis. The divergent validity of the CCT was assessed by comparing the Cognitive Index between the MCI and dementia groups. For the reliability test, we assessed internal consistency of the Cognitive Index by Cronbach’s alpha coefficient. ROC analysis was used to examine the diagnostic performance of the Cognitive Index in discriminating patients with dementia. The cut-off value of Cognitive Index was calculated based on the Youden’s Index (Sensitivity+Specificity-1). When the Youden’s Index reached the maximum, the cut-off value was obtained. The effects of age and educational level on the diagnostic performance of the Cognitive Index were also tested by ROC analysis.
Sample size
The sample size was calculated with PASS15. For diagnostic analysis, the sample size was calculated based on the estimation of ROC curve [26]. Estimating an AUC area of 0.92, an MCI/dementia ratio of 1.5, power of 0.8, and alpha of 0.05, the estimated sample size was 90. For correlation analysis, the sample size was estimated based on confidence intervals for Spearman’s rank correlation [27]. The confidence level was 0.95, the width of confidence interval was 0.2, the correlation coefficient estimate was 0.75. It was calculated that at least 100 patients were needed. Considering that dementia patients may have a higher dropout rate, 140 patients were finally recruited.
RESULTS
The median MMSE scores for the MCI group and the dementia group were 28.0 (interquartile range [IQR], 3.0) and 18.0 (IQR, 4.0), respectively. Median scores for the MCI group and dementia group on the MoCA were 22.0 (IQR, 4.0) and 10.5 (IQR, 6.0), respectively and the Cognitive Index were 90.4 (IQR, 14.1) and 51.4 (IQR, 27.9), respectively (Table 2). The Cognitive Index for patients with MCI was statistically significantly higher compared with the dementia group (Wilcoxon test, p < 0.001). The scores for the five cognitive domains in the CCT (thinking, perception, attention, memory, and executive function) differed significantly between the two groups (p < 0.001 for all comparisons) (Fig. 2). Patient age was weakly inversely correlated with the Cognitive Index (Spearman’s rho, –0.227; p = 0.014), and years of education was weakly positively correlated with the Cognitive Index (Spearman’s rho, 0.333; p < 0.001). Patient sex did not affect the Cognitive Index (Wilcoxon test, p = 0.579).
Cognitive assessments

Cognitive Index scores for each cognitive domain in the MCI and dementia groups. Between-group differences were analyzed using Wilcoxon’s test.
To confirm the convergent validity of the CCT, we examined the correlation between the Cognitive Index and neuropsychological assessment scores using Spearman’s correlation analysis. This showed that the Cognitive Index was strongly correlated with both MoCA (rho = 0.812, p < 0.001) and MMSE (rho = 0.694, p < 0.001) scores. Next, we examined the internal consistency by computing Cronbach’s alpha coefficient for the Cognitive Index among five cognitive domains. The Cronbach’s alpha was 0.936, indicating excellent internal consistency of the Cognitive Index.
Next, we assessed the diagnostic accuracy of the Cognitive Index for discriminating patients with dementia (Fig. 3). The ROC AUC was 0.943 (95% Confidence Interval (CI): 0.904–0.982; p < 0.001), with a sensitivity of 83.3% (95% CI: 72.1%–94.6%) and a specificity of 91.9% (95% CI: 85.7%–98.1%). The optimal cut-off point was 67.16. Because patient age and educational level affected the Cognitive Index score, we assessed diagnostic accuracy in patients divided into subgroups based on these demographic characteristics. For patients less than 60 years old (N = 27), the optimal cutoff point was 72.24, with a sensitivity of 1.000 and a specificity of 1.000, whereas in patients≥60 years old (N = 89), the cutoff point was 64.44, with a sensitivity of 78.1% (95% CI: 63.8%–92.4%) and specificity of 91.2% (95% CI: 83.9%–98.6%) (AUC = 0.921, p < 0.001, 95% CI: 0.866–0.975). This is consistent with our finding that increasing age negatively affected the Cognitive Index. Next, we divided patients into two groups based on having>9 or≤9 years of education. In the less-educated group (N = 42), the cut-off point was 66.23, with a sensitivity of 82.6% (95% CI: 67.1%–98.1%) and specificity of 84.2% (95% CI: 67.8%–100%) (AUC = 0.870, p < 0.001, 95% CI: 0.760–0.979), whereas, in the more-educated group (N = 74), the cut-off point was 72.08, with a sensitivity of 89.5% (95% CI: 75.7%–100%) and specificity of 92.7% (95% CI: 85.9%–99.6%) (AUC = 0.969, p < 0.001, 95% CI: 0.935–1.000). This was also consistent with our previous finding that educational level was positively correlated with the Cognitive Index.
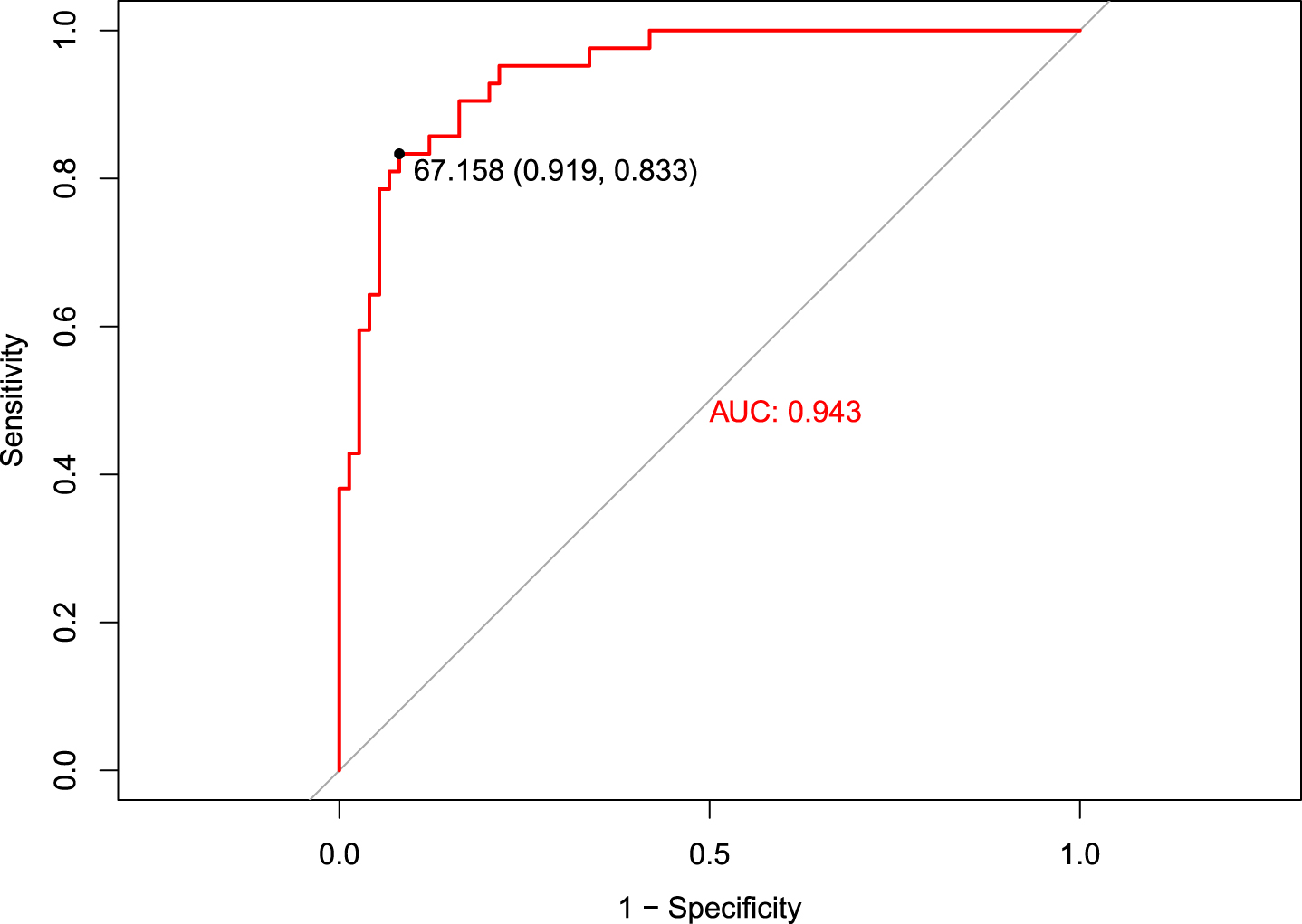
Ability of the Cognitive Index to discriminate patients with dementia evaluated using ROC analysis.
DISCUSSION
Patients with cognitive impairment suffer progressive cognitive decline after the onset of symptoms [3]. Therefore, monitoring cognitive status can provide valuable information for clinicians and caregivers to adjust disease management. There is a growing trend to use CCT as an alternative intervention in patients with cognitive impairment; thus, in this study, we assessed the validity and reliability of CCT as a cognitive assessment tool [15, 28]. To ensure that the performance of the patients in the study on the CCT reflected actual cognitive status, we only included patients who completed training tasks covering all five cognitive domains in the first week in the analysis. Unlike studies that screen patients with MCI from healthy populations, our study assessed cognitive status in patients with cognitive impairment who were diagnosed with MCI or dementia.
The validity of digital technology-based cognitive assessments in patients with cognitive impairment has been an active area of study over the past few decades. Speech performance and finger dexterity were found to be useful tools to distinguish older healthy people, patients with MCI and patients with dementia [29, 30]. However, these studies were limited to evaluating only a single performance (i.e., speech or finger dexterity) to assess cognitive ability. Digital-based cognitive batteries have also been developed to enable comprehensive assessments of cognition [31, 32], but the ones developed so far have been considered too time consuming or unreliable to become broadly adopted for self-administered home-based cognitive monitoring. In contrast, CCT is more entertaining and better tolerated by patients and clinicians, making it more suitable for longitudinal cognitive monitoring.
We selected a CCT program containing 15 games targeting multiple cognitive domains and recruited a relatively large sample size of patients to validate the feasibility and accuracy of CCT for cognitive monitoring. The convergent validity of the CCT-generated Cognitive Index demonstrated that this CCT is a promising tool for assessing cognitive abilities in patients with cognitive impairment. Thompson et al. evaluated game performance and neuropsychological assessments of 29 old participants [33] and found significant moderate correlations between several game performance and neurocognitive test scores; specifically, significant correlations were detected between picture game and visual memory test performance, between word game and verbal IQ and verbal learning test performance, and between number game and reasoning solving test performance. Wang et al. developed a game-based cognitive assessment tool that correlated strongly with the MMSE (r2 = 0.92) and Cognitive Abilities Screening Instrument (CASI) (r2 = 0.90) [11]. However, this game-based cognitive assessment tool was not designed for cognitive training. Zygouris et al. applied VR-based cognitive training for cognitive monitoring, and they identified significant correlations between the mean duration of VR training and the Functional Cognitive Assessment Scale (FUCAS; r = 0.645), the Test of Everyday Attention Item 4 – raw score (TEA4r; r=–0.617), and the Rey–Osterrieth Complex Figure Test – pattern copying (ROCFT1; r=–0.570) [22]. Our results indicate that the Cognitive Index calculated by the average performance of patients on our CCT battery is a valid method to assess cognitive status. The reliability of internal consistency was confirmed by calculating Cronbach’s alpha coefficient for patient performance on each of the different cognitive domains evaluated in the CCT.
We found a significant difference in the Cognitive Index of patients with MCI compared with patients with dementia, and the CCT-derived Cognitive Index showed good ability to discriminate patients with dementia (sensitivity, 83.3%; specificity 91.9%; AUC = 0.943). Recently, Oliva and Losa validated a computerized cognitive assessment tool for its ability to differentiate MCI from dementia, and it achieved sensitivity and specificity of 95.5% and 48.5%, respectively, with an AUC = 0.726 [34]. The low specificity could result from the fact that they only administered a single test or from the test having a low level of difficulty. When patients were subdivided into groups based on age and educational level, we found that cut-off values were higher for younger patients (<60 years old) as well as higher for patients with>9 years of education, which was consistent with our finding that age and educational level were negatively and positively correlated with the Cognitive Index, respectively. The sensitivity and specificity of the Cognitive Index exhibited substantial variability in subgroup analyses, likely attributable to the limited sample size within the subgroups. Particularly, the younger group only contained 27 patients and the AUC may not reflect the real situation.
The use of performance on cognitive training exercises to determine cognitive ability has been explored. Tong et al. developed a serious game that mimicked the Go/No-Go Discrimination Task and used response time as the measure of game performance [35], and they found that game performance correlated significantly with the MoCA and MMSE (r=–0.339 and –0.558, respectively). Wiloth et al. developed Physiomat-Trail-Making Tasks (PTMTs) to test the complex performance of motor and cognitive functions, and they found the complex PTMTs correlated well with MMSE (r = 0.66). In our study, performance was assessed for tasks covering 5 different cognitive domains and the Cognitive Index was more strongly correlated with neurocognitive assessment scales compared with the previous research.
One limitation of this study is that healthy individuals were not evaluated; thus, whether the Cognitive Index of the CCT tested in this study is suitable for assessing cognitive function in people without objective cognitive impairment requires further investigation. However, the purpose of this study is to investigate whether cognitive training is a suitable tool for cognitive monitoring in patients with cognitive impairments; thus, the mainly conclusion of this research would not be mitigated. In the research, the participants in our study were individuals who voluntarily chose to participate, which may not represent the entire population. The use of a highly select self-selected sample introduces potential limitations and may have resulted in selection bias. Further, the subgroup analyses were underpowered due to the relatively small sample sizes. Besides, most participants included in our study had less advanced cognitive impairment. This is primarily because our study focused on individuals who underwent cognitive training, which was mainly designed for those with mild cognitive impairment and early dementia. The patients with dementia in our research were relatively younger. This can be attributed to two main reasons. Firstly, the patients were recruited from the department of neurology, where individuals with early onset dementia were more likely to seek consultation compared to the geriatric department. Another contributing factor is younger patients were more willing to seek medical treatment. The selection bias may limit the generalization of our conclusion. In addition, our conclusions are limited by the fact that we only determined the Cognitive Index after one week of CCT, and future studies should explore the validity and reliability of the Cognitive Index after longer training periods as well as determine the potential prognostic value of generating longitudinal data with this tool.
In conclusion, we administered a CCT to patients with MCI or dementia and examined the validity and reliability of its Cognitive Index to assess cognitive status and to discriminate patients with dementia. Our results suggest that a CCT-derived Cognitive Index can be used to detect cognitive ability and may be an accessible tool for more personalize clinical management of patients with cognitive impairment.
Footnotes
ACKNOWLEDGMENTS
The study was completed in the collaboration with Peking University Clinical Research Institute, Peking University First Hospital and Beijing Wisdom Spirit Technology Co., Ltd. The authors thank all the patients volunteered in this research.
FUNDING
This work was supported by the National Key Research and Development Program of China (2022YFC3602600), National Natural Science Foundation of China (82220108009, 81970996), and STI2030-Major Projects (2021ZD0201801).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data is not available because the participants of this study did not agree for their data to be shared publicly.