
Abstract
Active x-ray collimation is well adopted in radiography and fluoroscopy for radiation dose reduction and image quality improvement. The application of this concept in computed tomography (CT) is significantly limited due to the truncation of projection data. Generally, an internal field of view (FOV) inside an imaging object cannot be exactly reconstructed only from the truncated projection data. Recent research shows that given some prior information of the FOV image, interior tomography can provide a unique and stable solution for image reconstruction of an internal FOV. The objective of this study is to evaluate the performance of interior reconstruction based on patient datasets obtained from a clinical CT scanner with dual x-ray tubes, which simultaneously gives full projections and truncated projections. Image reconstructions are performed from full and truncated projection data for the comparison of image quality, respectively. The reconstructed CT images were reviewed by a radiologist and a resident. The evaluation results of two observers showed that CT images reconstructed with truncated projections met clinically diagnostic requirements and were comparable to clinical images. This study demonstrates that with the development of interior tomography, active x-ray collimation in the imaging plane can be readily employed in CT imaging to further reduce patient radiation and improve image quality.
Keywords
Introduction
Dose-reduction techniques commonly used in x-ray imaging include active collimation, automatic exposure control, optimal tube potential, and the use of individual protocols [1–3]. Actively collimating the x-ray to the volume of interest reduces the overall integral dose to the patient and thus minimizes the radiation risk. Less volume irradiated by x-rays also helps to decrease x-ray scatter incident on the detector, improving subject contrast and image quality. This concept has been well adopted in radiography and fluoroscopy projection imaging but not in computed tomography (CT). Much research has been conducted over the years with respect to CT radiation dose reduction [4–12]. Among those, very limited effort has been focused on the use of collimation, especially in the imaging plane. There is a great potential to further reduce CT radiation dose by combining active collimation with other available techniques.
The key issue with the use of collimation in the CT imaging plane is its image quality. In CT, collimated x-rays only go through a region of interest (ROI) inside the imaging object, which would result in the truncation of projection data. Traditional CT theory targets image reconstruction for a whole object without any truncation of projections. When a general CT algorithm (e.g., FBP) is applied to truncated projections for image reconstruction, bright shading artifacts are produced near the edge of the truncation, overlapping features in the ROI. Truncation artifacts become more pronounced as larger amounts of the projections are truncated [13].
The conventional wisdom is that an interior ROI cannot be exactly reconstructed from only truncated projection data measured through the ROI. This historic concept has contributed to the current CT architectures whereby the detectors are sufficiently wide to cover a transaxial section fully. The specific algorithm employed in this study is called interior tomography (IT) [14, 15], in which an internal ROI is irradiated with x-rays only through the ROI to recover the ROI image exactly. IT overcomes the transverse data truncation innovatively and potentially reduces the integral dose deposited in the patient. Recent analytical and experimental results showed that the interior problem indeed permits a unique and stable solution if the ROI image is piecewise polynomial, which is a general image model [16–18]. Rigorous theoretical analysis on the uniqueness and stability of interior reconstruction has been reported based on the assumption of piecewise constant or polynomial image on an ROI [19–26].
The objective of this study is to evaluate image quality of CT images reconstructed using interior tomography and projection data of patients directly from a clinical CT scanner. Two sets of projections, full projections and truncated projections, were used for the validation.
Methods and materials
This retrospective study was approved by the institutional review board at the University of Kentucky. Raw projection data were directly retrieved from patients who were scanned in a Siemens Dual-Source CT scanner (DSCT, Somatom Definition, Siemens Healthcare, Erlangen, Germany). A CT protocol for prospective cardiac imaging was selected. The scan parameters are provided in Table 1. To illustrate the effectiveness of the image reconstruction algorithm, those patients who were scanned with “sequential (axial) mode” were selected to simplify image reconstruction. For this pilot study, projections were retrieved from 6 patients.
Scan parameters for CT acquisition
Scan parameters for CT acquisition
For this scan protocol, both Tube A and Tube B were used. Tube A provided a full FOV (50 cm) of patients without truncation, while Tube B provided a small scan FOV (26 cm) with truncated projection data, as shown in Fig. 1. In routine practice, the mixed projection data from Tube A and Tube B are used to generate CT images.
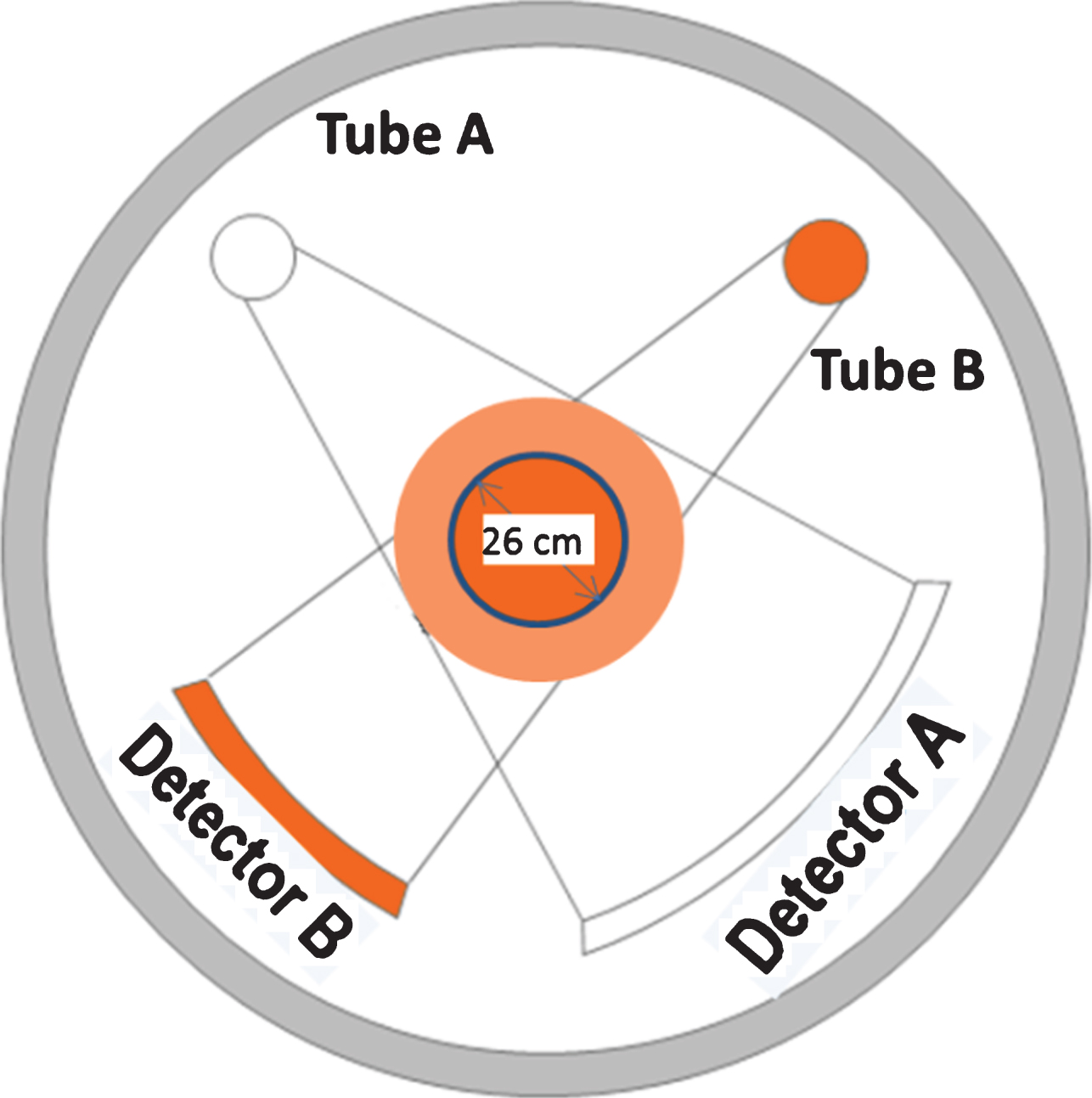
Diagram of Dual Source CT scanner used for simultaneous acquisition of full projections (FOV of 50 cm) and truncated projections (FOV of 26 cm).
In our study, we used projection data from Tube A and Tube B separately for image reconstruction. Tube B data was to simulate when the x-ray was collimated in the imaging plane to a small FOV. Tube A images and Tube B images were generated using filtered back projection (FBP) and iterative interior tomography, respectively.
A board-certified radiologist with 10 years of experience in thoracic CT imaging and a senior resident reviewed the images using the picture archiving and communication system (PACS) viewer (Barco, GA, USA). The observers were blinded to the image reconstruction algorithms. The reading time was not limited. They assessed the images using a four-point subjective scale as follows: 4 (Excellent): no obvious image noise and clear, providing useful information; 3 (Good): slight image noise but still clear, providing sufficient diagnostic information; 2 (Fair): image noise was present, providing acceptable diagnostic information; 1(Poor): very noisy image, yielding insufficient diagnostic information.
Weighted CTDI (CTDIw) were calculated with a PMMA CT body phantom to demonstrate radiation dose reduction. The phantom was scanned in “service” mode in which the acquisition parameters can be set up to be the same for Tube A and Tube B, and the tubes can be tested separately. The acquisition parameters were 120 kV, 300 mAs, rotation time of 1 sec, and collimation of 32×0.6 mm.
Figure 2 shows the reconstructed images with full scan FOV projections obtained from Tube A, while Fig. 3 shows the reconstructed images with truncated projections corresponding to Tube B. CT images were reconstructed using an iterative interior reconstruction technique and FBP, respectively. Clinical images from the CT scanner were also presented to the observers. The clinical images were reconstructed using FBP with a kernel of B26f, a displayed FOV of 18 cm, and a slice thickness of 0.75 mm. For comparison, window level/width settings are approximately the same.
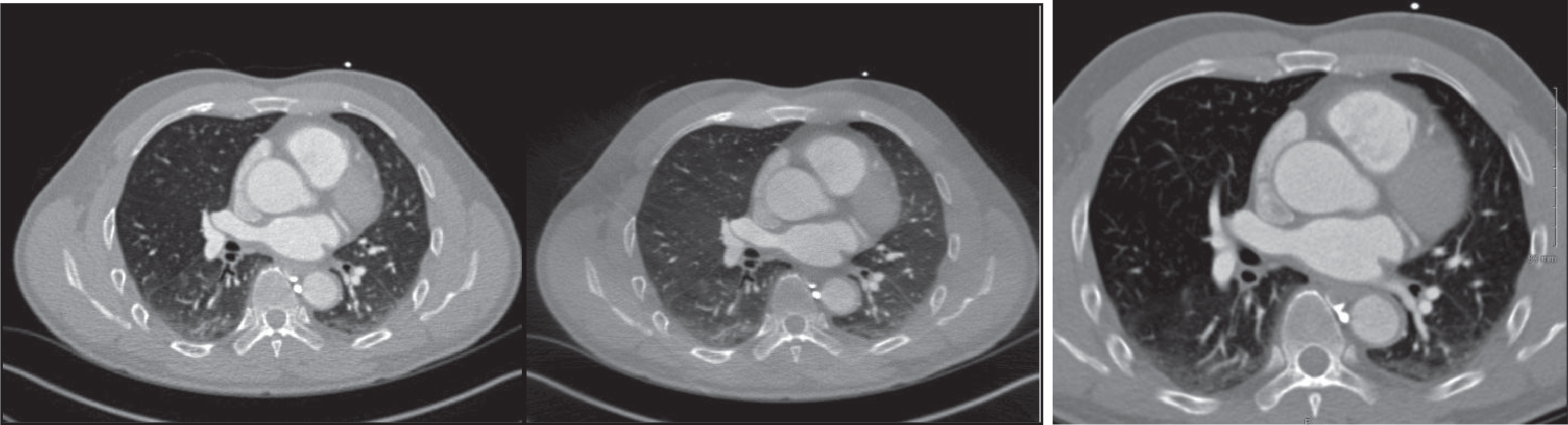
An example of Tube A images reconstructed using iterative interior tomography (Left) and FBP (Middle) with full scan FOV projections, respectively. The right image shows clinical image from the CT scanner, which were reconstructed using FBP with a B26f kernel, a displayed FOV of 26.3 cm, and a slice thickness of 0.75 mm. Window level/width settings are approximately the same.

An example of Tube B images reconstructed using iterative interior tomography (Left) and FBP (Middle) with truncated projections, respectively. The right image shows clinical image from the CT scanner, which were reconstructed using FBP with a B26f kernel, a displayed FOV of 18 cm, and a slice thickness of 0.75 mm. Window level/width settings are approximately the same.
The observers’ evaluation is reported in Table 2. There is no obvious difference observed between the score for Tube B, images with truncated projections, and those for Tube A, images reconstructed with full FOV projections. There were substantial inter-observer agreements regarding the visual score.
Score of CT images reconstructed with truncated projections (Tube B) and non-truncated projections (Tube A), compared with clinical CT images
CTDIw for Tube A (scan FOV of 50 cm) and Tube B (scan FOV of 26 cm) are 20.5 mGy and 18.4 mGy, respectively. For the same acquisition parameters, Tube B delivers approximately 10% less radiation compared to Tube A for a standard 32 cm PMMA body phantom.
Our validation study shows that CT images reconstructed using interior tomography can meet clinical diagnostic requirements. In theory, CT images reconstructed with truncated projections should show superior image quality compared to those with full projections, due to decreased scatter radiation. However, this may be only true when the acquisition parameters are the same. In our study, a pre-set cardiac examination protocol was selected. In this clinical protocol, Tube B used 140 kV while Tube A used 80 kV. With higher kV, Tube B images lost contrast to some extent. In addition, because patients were simultaneously scanned with Tube A and Tube B, the same amount of scattered radiation was added to all projection data. Therefore, it is not surprising to see Tube B images are inferior to Tube A images. It would be a different scenario if active collimation is used, where scattered radiation will be significantly reduced and acquisition parameters can be selected.
Differences in the reconstruction kernel and slice thickness also influence image quality. We reconstructed CT images off-line. With this limitation, we only reconstructed images with a slice thickness of 0.6 mm. These images look ‘noisy’ compared to those with thicker slice thicknesses such as 0.75 mm. We cannot exactly match the FBP kernel “B26f” in the CT scanner either. In addition, CT numbers between the clinical images and those reconstructed off-scanner images vary, due to the variation of linear attenuation coefficients for corrections. This variation has a minimal effect on the current study to examine image quality since relatively equivalent brightness could be achieved. The variation in CT numbers can be addressed if the interior tomography reconstruction algorithm is applied in the CT scanner.
Our simple phantom study shows more than 10% dose reduction for a standard 32 cm PMMA CT body phantom. More radiation dose reduction would be expected for large size patients. As shown in Fig. 4, assuming a patient is scanned with a partial scan FOV (e.g., 50% of the full FOV in this example), radiation dose reduction for peripheral organs and other tissues can reach up to 50%, based on a Monte Carlo simulation (The GMctdospp program, Technische Hochschule Mittelhessen, Germany) with typical physical aspects of a CT scanner. The radiation dose reduction strongly depends on the scan FOV.
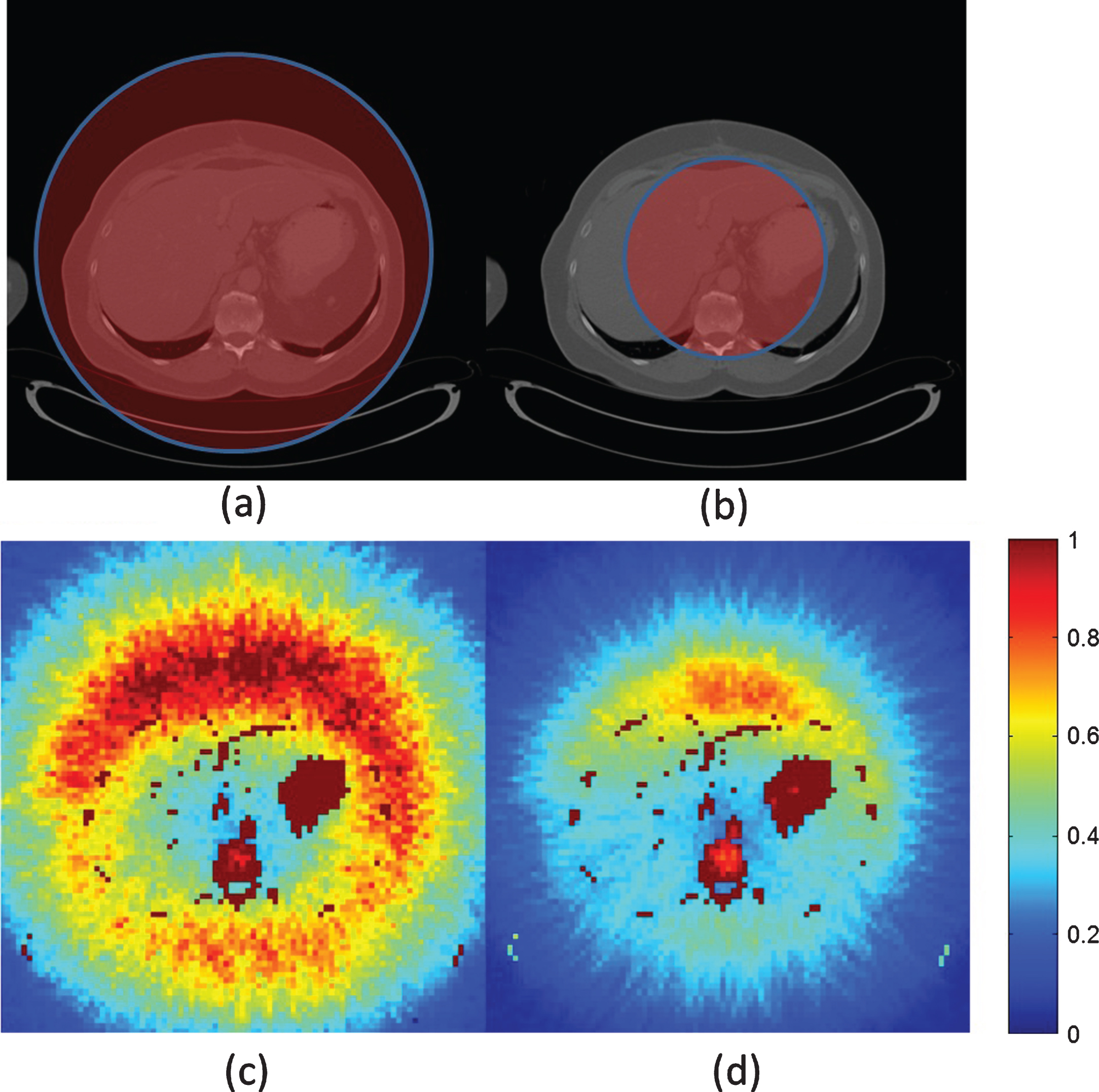
Monte Carlo based investigation of dose reduction capability with the active collimation. (a) and (b) are the CT images of the patient in which the area being irradiated at all angles are marked by red, and (c) and (d) are the dose map of the two cases, respectively. Note the substantial reduction of radiation dose to the peripheral organs. The color bar indicates the dose normalized by the maximum dose. Red indicates high dose while blue indicates low dose.
With interior tomography, active collimation can be readily employed in CT imaging to further reduce patient radiation and/or improve image quality. A practical example for the use of active collimation is CT imaging of obese patients. For obese patients, most adipose tissue is subcutaneous which is of less clinical relevance. However, this layer of adipose tissue significantly boosts the radiation dose during CT image procedures as well as degrades the image quality with increased scatter radiation. Other potential applications include cardiac imaging, which delivers the largest radiation dose to a patient of any single CT examination. The use of active collimation may also potentially reduce radiation dose to sensitive organs such as the breast.