
Abstract
OBJECTIVES:
To explore the potential added value of dynamic contrast enhanced ultrasound (DCE-US) using VueBox® software for the diagnosis of small solid thyroid nodules (≤1.0 cm).
PATIENTS AND METHODS:
This prospective study was approved by the institutional review board and it was performed at two hospitals from January 2020 to October 2020. B mode ultrasound and contrast enhanced ultrasound (CEUS) images were obtained for 79 small solid thyroid nodules (≤1.0 cm) confirmed by ultrasound-guided fine needle aspiration cytology results in 79 consecutive patients (55 women and 24 men, median age: 41 years). The CEUS time-intensity curves (TICs) of thyroid nodules and surrounding parenchyma were created by VueBox® software (Bracco, Italy). The CEUS quantitative parameters were obtained after curve fitting. The diagnostic performance of CEUS and DCE-US was evaluated and compared. The weighted kappa statistic (κ) was performed to assess the interobserver agreement and consistency between the diagnosis of CEUS and DCE-US.
RESULTS:
Among the 79 thyroid nodules, 56 (70.9 %) were malignant and 23 (29.1 %) were benign lesions. Hypoenhancement during the arterial phase of CEUS was associated with malignancy (P < 0.001), with an AUC of 0.705 (sensitivity 71.4 %, specificity 69.6 %). Among all CEUS quantitative parameters, the peak enhancement (PE), wash-in rate (WiR), and wash-out rate (WoR) of DCE-US in malignancies were significantly lower than those in benign nodules (P = 0.049, P = 0.046, and P = 0.020, respectively). The area under the receiver operating characteristic curves (AUCs) of PE, WiR, and WoR were 0.642 (sensitivity 65.2 %, specificity 67.9 %), 0.643 (sensitivity 43.5 %, specificity 91.1 %), and 0.667 (sensitivity 69.6 %, specificity 69.6 %) in differentiation between benign and malignant small solid thyroid nodules (≤1.0 cm), respectively. Comparing the quantitative parameters of DCE-US between small solid thyroid nodules and surrounding normal thyroid parenchyma, the PE, WiAUC, WiR, wash-in perfusion index (WiPI), WoAUC, WiWoAUC, and WoR of the nodules were significantly lower than those of normal thyroid tissue (P = 0.008, P < 0.001, P = 0.037, P = 0.009, P = 0.003, P = 0.002, P = 0.049, respectively). A total of 16 (20.3 %) nodules showed isoenhancement during the arterial phase of CEUS, while the median PE ratio of surrounding tissue and thyroid nodules was 1.70 (IQR: 1.33–1.89).
CONCLUSIONS:
VueBox® is a helpful tool for the evaluation of dynamic microvascularization of thyroid nodules, and DCE-US using VueBox® perfusion analysis could provide added values for differential diagnosis of small solid thyroid nodules (≤1.0 cm).
Keywords
Introduction
Malignant lesions are detected in 10 % of patients who present with thyroid nodules [1]. Among these, more than 90 % are well-differentiated papillary thyroid carcinoma (PTC), which is asymptomatic with a survival rate greater than 95 % [2]. In recent years, microwave (MW) ablation was recommended to be a safe and effective way to treat small thyroid malignant lesions as well as large benign thyroid nodules [3–5]. Before MW treatment, it is of vital importance to make a precise diagnosis of small thyroid nodules [5].
Contrast enhanced ultrasound (CEUS) of thyroid nodules is an effective technique for evaluating the microvascular perfusion, which could be helpful in obtaining a more precise and reproducible image of lesion before MV ablation [6–9]. According to current guidelines [10], hypoenhancement is the most accurate CEUS feature of thyroid malignancies, with a sensitivity, specificity, and accuracy of 82.0 %, 85.0 %, and 84.0 % respectively. Most benign thyroid nodules tend to show a regular perfusion pattern, whereas malignant nodules typically have a more chaotic pattern [11]. However, the variable specificities may be caused by the different sizes of thyroid nodules. Small thyroid malignancies may lack vascularization and exhibit different vascular diameters and shapes, resulting in increased difficulty in distinguishing malignant and benign small thyroid nodules [12–14]. A correct and reliable application of qualitative CEUS depends on the experience and visual interpretation of the operator, which limits its widespread application as a diagnostic procedure [7].
Dynamic contrast-enhanced ultrasound (DCE-US) is a quantitative imaging technique based on CEUS images. Reproducible perfusion parameters can be obtained by DCE-US to evaluate the dynamics of thyroid nodule microvascular perfusion [15], which can be more easily obtained and interpreted by the operator, regardless of the operator’s level of experience. Previously, DCE-US applications in the thyroid included determining different perfusion characteristics of adenomas and carcinomas of the thyroid gland [16] and differentiating whether the TI-RADS III nodule is an early-stage malignancy [10]. However, none has been published on the added value of the quantitative parameters of DCE-US in determining the perfusion pattern of small thyroid nodules, especially before MW treatment.
The purpose of our study was to investigate the added value of DCE-US using VueBox® (Bracco, Milan, Italy) external software for the diagnosis of small (≤1.0 cm) thyroid nodules.
Patients and materials
Patients
This prospective study was approved by the institutional review board (B2020-425), and the informed consent of patients was waived. This study was performed at two hospitals from January 2020 to October 2020.
The inclusion criteria were as follows: 1) patients (age > 18 years) with small solid thyroid lesions (≤1.0 cm) detected on B mode ultrasound (BMUS); 2) absence of BMUS-based gross extrathyroidal extension; 3) absence of lymph node or distant metastasis; 4) patients who received CEUS examinations one week before biopsy; 5) DICOM format of CEUS clips longer than 120 sec was available; and 6) the final diagnosis was confirmed by ultrasound-guided fine needle aspiration (FNA) and cytology results, and benign results were confirmed by repeated FNAs [17].
The exclusion criteria were as follow: 1) the thyroid nodule was not visible on a BMUS scan; 2) patients lacked CEUS DICOM video; and 3) the patients could not cooperate during CEUS.
Ultrasound examinations procedure
All ultrasound examinations were performed by experienced examiners with two high resolution ultrasound machines (LOGIQ E9 [GE Healthcare, Solingen, Germany], equipped with an L9-3 linear-array transducer; Acuson Sequoia [Siemens Healthineers, Erlangen, Germany], equipped with an L9-4 linear-array transducer).
BMUS features were recorded for each thyroid nodule including the location, size (the maximal diameter on BMUS), echogenicity (compared to the surrounding normal thyroid tissue, classified as hypoechoic, or mix-echoic if the echogenicity was mainly isoechoic or hyperechoic), shape (wider-than-tall or taller-than-wide shape was assessed by measurements), margin (smooth or irregular) and with or without punctate echogenic foci. The nodules were classified following the American College of Radiology (ACR) Thyroid Image Reporting and Data System (TI-RADS) classification [18].
CEUS was performed after i.v. injection of 1.2–2.4 ml sulfur hexafluoride microbubbles (SonoVue®, Bracco, Milan, Italy) via the cubital vein, followed by a 5 ml saline flush. Two radiologists with more than 15 years of experience in thyroid CEUS performed the CEUS examinations with awareness of the patients’ clinical histories. A clip at least 2 minutes in length displaying the enhancement process of the thyroid nodule was recorded continuously without movement of the transducer. The CEUS data were exported in DICOM format as a cine loop. The intensity of the nodules on CEUS was recorded and observed [10, 19]. Two radiologists reviewed the CEUS images independently, discussed any divergent interpretations, and then reached a consensus.
DCE-US quantitative analysis
VueBox® is an off-line contrast perfusion quantification analysis computer software for CEUS [20]. The digitally stored DICOM cine loops were analysed by one radiologist (with 10 years of experience in thyroid CEUS) who was blinded to the patients’ clinical and other imaging and pathological results. The CEUS clips were observed dynamically. Regions of interest (ROIs) were placed in the suspected lesions and the surrounding normal thyroid parenchyma as a reference region. The time-intensity curves (TICs) were fitted and linearized, which displayed the average intensity in ROIs as a function of time, reflecting the transit of the contrast microbubbles.
After curve fitting, the fitting results were considered credible when the quality of fit was > 75 %. Various DCE-US quantitative parameters were created (Fig. 1), including peak enhancement (PE), wash-in rate (WiR, the maximum slope of the TIC represented as a tangent at the ascending part of the curve), wash-out rate (WoR, the minimum slope of the curve, represented as a tangent at the descending part of the curve), wash-in area under the curve (WiAUC, area under the TIC from time of arrival to the peak enhancement), wash-out AUC (WoAUC, the area under the TIC from the peak enhancement to the end of the curve), wash-in and wash-out AUC (WiWoAUC, the area under the TIC), rise time (RT), wash-in perfusion index (WiPI, WiAUC/RT), mean transit time (mTT), time to peak (TTP), fall time (FT) [21].
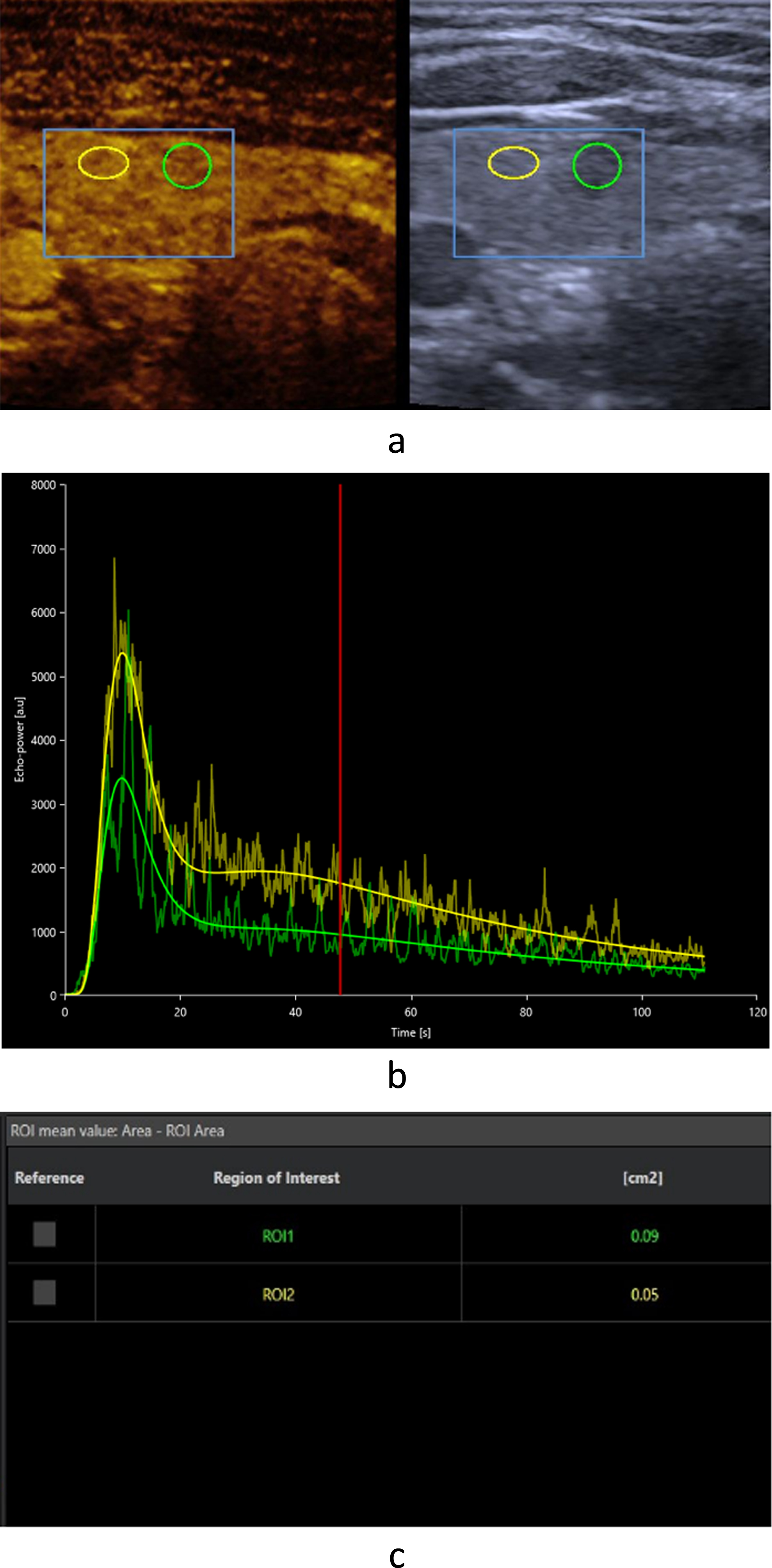
CEUS (contrast enhanced ultrasound) perfusion imaging of a small pathologically proven PTC (papillary thyroid carcinoma). Two ROIs (regions of interest) were manually set inside the target lesion (green ROI) and in the surrounding normal thyroid parenchyma (yellow ROI) as a reference region (a). TIC (time-intensity curves) analysis of the ROIs showed that the peak enhancement with lower levels at the PTC in comparison with the surrounding thyroid tissue (b). After curve fitting, various CEUS perfusion parameters could be obtained (c).
All the CEUS parameters were recorded and compared between thyroid nodules and surrounding parenchyma.
Continuous variables are expressed as the means with standard deviations or medians and interquartile ranges (IQRs). Groups were compared using the student t-test or Mann-Whitney U-test depending on the distribution. The diagnostic efficiency of the CEUS and DCE-US was assessed by correlation to pathological results, using accuracy, sensitivity, specificity, and area under receiver operating characteristic (ROC) curve analysis, with 95 % confidence intervals (CIs). The weighted kappa statistic (κ) was performed to assess the consistency between the diagnostic performance of CEUS and DCE-US; and the interobserver agreement between the two radiologists regarding the CEUS enhancement patterns of the nodules. The κ= 0 0.20, slight agreement; κ= 0.21 0.40, fair agreement; κ= 0.41 0.60, moderate agreement; κ= 0.61 0.80, substantial agreement; and κ= 0.81 1.00, almost perfect agreement [22]. All data were calculated using the software program SPSS Statistics 22.0 (IBM, Armonk, USA) and GraphPad Prism 9 (GraphPad Software, Inc.). P value < 0.05 was considered statistically.
Results
Characteristics of the patients and thyroid nodules
A total of 79 patients (55 women and 24 men, median age: 41 years [IQR: 35 51]) with 79 thyroid nodules (median size: 0.6 cm [IQR: 0.5 0.8]) were included. Thirty nodules (38.0 %) were located in the left lobes, while 49 nodules (62.0%) were located in the right lobes.
Among 79 thyroid nodules, 56 (70.9 %) were malignant and 23 (29.1 %) were benign. The specific pathological types were as follows: the malignancies were all PTCs; the benign nodules included 1 inflammatory nodule, 13 Hashimoto’s thyroiditis, 7 nodular goiters, and 2 hemorrhagic colloid nodules.
B-mode ultrasound (BMUS) characteristics
In the BMUS image, the majority of solid thyroid nodules displaced hypoechogenicity (83.5 %, 66/79), irregular margins (74.7 %, 59/79), and wider-than-tall shapes (51.9 %, 41/79). More than half of the nodules had punctate echogenic foci (50.6 %, 40/79). Among the 79 nodules, 52 were classified as TR 5 by the ACR TI-RADS, 26 were classified as TR 4, and only one was classified as TR 3.
Diagnostic performance of CEUS
The two radiologists had an almost perfect agreement, with a κ of 0.824±0.059 for CEUS intensity assessment. A total of 47 (59.4 %) nodules showed hypoenhancement, 16 (20.2 %) isoenhancement, and 16 (20.2 %) hyperenhancement during the arterial phase of CEUS.
Among the 56 thyroid malignancies, 40 (71.4 %) showed hypoenhancement, 8 (14.3 %) isoenhancement, and 8 (14.3 %) hyperenhancement during the arterial phase of CEUS. While among the 23 benign thyroid nodules, 7 (30.4 %) had hypoenhancement, 8 (34.8 %) isoenhancement, and 8 (34.8 %) hyperenhancement during the arterial phase of CEUS. Hypoenhancement on CEUS was associated with malignancy (Mann-Whitney U = 908.0, P < 0.001).
The area under the ROC (AUC) of CUES was 0.705 (95 % CI 0.576–0.834, P = 0.004) for hypoenhancement during the arterial phase for diagnosis of malignant thyroid nodules. Application of this cut-off resulted in an accuracy of 70.9 %, a sensitivity of 71.4 % (95 % CI 58.5 81.6), and a specificity of 69.6 % (95 % CI 49.1 84.4).
Diagnostic performance of DCE-US quantitative parameters
Comparing the quantitative parameters of DCE-US between small thyroid malignant and benign nodules, the PE, WiR, and WoR in malignancies were significantly lower than those in benign nodules (P < 0.05) (Table 1). The TIC analysis indicated that compared with the benign nodules, the malignancies showed relatively slow and lower enhancement during the arterial phase.
Dynamic contrast enhanced ultrasound (DCE-US) quantitative parameters between benign and malignant thyroid nodules
Dynamic contrast enhanced ultrasound (DCE-US) quantitative parameters between benign and malignant thyroid nodules
*A P value < 0.05 was regarded as statistically significant. s: time-related parameters in seconds. a.u.: signal intensity parameters in arbitrary units.
The AUC of the PE was 0.642 (95 % CI 0.491–0.793, P = 0.049), and the best cut-off value for predicting malignant nodules was 2010.2 a.u. (sensitivity 65.2 %, specificity 67.9 %). The AUC of the WiR was 0.643 (95 % CI 0.494–0.793, P = 0.047), and the best cut-off value for predicting malignant nodules was 1305,4 a.u. (sensitivity 43.5 %, specificity 91.1 %). The AUC of the WoR was 0.667 (95 % CI 0.521–0.813, P = 0.020), and the best cut-off value for predicting malignant nodules was 289.4 a.u. (sensitivity 69.6 %, specificity 69.6 %) (Fig. 2).

ROC (Receiver operating characteristic) analyses of the diagnostic performance of the PE, WiR, and WoR (DCE-US quantitative parameters) for predicting the malignant thyroid nodules. The AUCs (Area under the ROCs) of the PE, WiR, and WoR were 0.642, 0.643, and 0.667, respectively.
CEUS and DCE-US for the diagnosis of malignant and benign thyroid nodules showed substantial agreement, with a κ of 0.631±0.112 for contrast agent perfusion assessment.
Comparing the quantitative parameters of DCE-US between small solid thyroid nodules and surrounding normal thyroid parenchyma, the PE, WiAUC, WiR, WiPI, WoAUC, WiWoAUC, and WoR of the nodules were significantly lower than those of normal thyroid tissue (P = 0.008, P < 0.001, P = 0.037, P = 0.009, P = 0.003, P = 0.002, P = 0.049, respectively). However, the RT, mTT, TTP, and FT were not associated with the presence of thyroid nodules (P = 0.708, P = 0.104, P = 0.422, P = 0.903, respectively).
A total of 16 (20.3 %) nodules showed isoenhancement during the arterial phase of CEUS, while their median PE was 887.3 a.u. (IQR: 502.1–3245.1), lower than that of the surrounding normal thyroid parenchyma on DCE-US. The median PE ratio of surrounding tissue and thyroid nodules was 1.70 (IQR: 1.33–1.89) (Fig. 3). Among these 16 nodules, the median PE of benign (2357.6 a.u. [IQR: 466.8 4025.2]) and malignant (2175.6 a.u. [IQR: 1461.3 3848.1]) nodules did not show a statistically significant difference (Mann-Whitney U = 26.0, P = 0.529).

A case of papillary thyroid carcinoma. B-mode ultrasound image showed a 0.5 cm solid, hypoechoic, taller-than-wide, irregular margin nodule in the right lobe of the thyroid (a). Contrast enhanced ultrasound image showed that the nodule was isoenhanced (arrows) during arterial phase (b). On Vuebox analysis, two separate ROIs were manually set inside the target lesion (green ROI) and in the surrounding normal thyroid parenchyma (yellow ROI) as a reference region (c). The TIC analysis indicated that comparing with the thyroid parenchyma, the nodule showed relatively lower enhancement during arterial phase. The peak enhancement of nodule was 904.0 a.u., while the surrounding parenchyma was 1504.3 a.u. (d).
In recent years, the incidence of PTC has increased significantly, especially for lesions≤1.0 cm [23]. Thermal ablation is a minimally invasive procedure of treating small thyroid malignancies that avoid removal of thyroid gland [24]. It is vital to achieve an accurate diagnosis before ablation. The diagnosis of thyroid nodules relies on ultrasound, which is used to identify thyroid malignancies based on suspicious BMUS features, including solid composition, hypoechoic, irregular margins, taller-than-wide shape, and microcalcifications [25]. In the present study, the majority of solid thyroid nodules displaced hypoechogenicity (83.5 %), irregular margins (74.7 %), and wider-than-tall shapes (51.9 %). More than half of the nodules had punctate echogenic foci (50.6 %). However, features of small thyroid nodules may overlap [26]. Furthermore, the identification of BMUS features of nodules depends on the operator’s experience [7].
CEUS can be used to assess thyroid nodules that cannot be evaluated by BMUS alone [27]. CEUS analysis uses SonoVue® to investigate microbubbles in microvessels, assessing their wash-in and wash-out kinetics. Therefore, it can be used to clarify the margins of nodules between the centre of nodules and surrounding tissue before ablation and guide ablation procedures [6, 29]. Various studies have shown that CEUS is highly sensitive for distinguishing between benign and malignant thyroid nodules [16, 31]. A statistically significant finding in our study was a hypoenhancement enhancement intensity for the detection of malignant nodules (P = 0.001), with an accuracy of 70.9 %, sensitivity of 71.43 %, and specificity of 69.57 %. This finding is in concordance with the data published by Chen et al. [32] where the hypoenhancement was considered to be a major contrast enhancement characteristic of malignancies, especially for thyroid nodules≤1.0 cm. The connective tissue between neovascular epithelia is not tight in small thyroid malignancies, and the cancerous vascular thyroid wall is thinner than the normal thyroid wall, resulting in an incomplete basement membrane and various irregular blood vessels. This may be the reason why the thyroid nodule enhancement is different from that of the benign nodules and surrounding normal thyroid parenchyma [32, 33]. However, overlapping enhancement features may occur in nodules as well. In this study, among the 56 thyroid malignancies, 40 (71.4 %) showed hypoenhancement, 8 (14.3 %) isoenhancement, and 8 (14.3 %) hyperenhancement during the arterial phase of CEUS. While among the 23 benign thyroid nodules, 7 (30.4 %) had hypoenhancement, 8 (34.8 %) isoenhancement, and 8 (34.8 %) hyperenhancement during the arterial phase of CEUS. Bartolotta et al. [13] concluded that overlapping features seem to confine the potential of CEUS in the characterization of thyroid nodules. Moreover, the perfusion pattern of small thyroid nodules could be difficult to analyse during the early arterial phase (10–15 s) of CEUS [10, 11], as they show a similar intensity of perfusion as the surrounding normal tissue in a very short time. CEUS for thyroid imaging could be seen as more helpful if additional quantitative parameters were provided.
To explore the potential added value of quantitative CEUS in the diagnosis of small thyroid nodules, VueBox® external software was used by DCE-US to assess cine loops of CEUS, which has been proven to have the potential for a better understanding of dynamic wash-in and wash-out processes of CEUS in various organs [15, 34–36]. For small thyroid nodules with indistinctive changes on CEUS features, which are invisible to operators, perfusion imaging with VueBox® can be used for the assessment of nodule microvascular perfusion to assist with diagnosis [11, 28]. A significant finding in the present study was that the PE, WiAUC, WiR, WiPI, WoAUC, WiWoAUC, and WoR of DCE-US in nodules were lower than those of the surrounding normal thyroid tissue. A total of 20.3 % (16/79) of nodules showed isoenhancement during the arterial phase of CEUS, while after curve fitting, the median PE ratio of surrounding tissue to thyroid nodules was 1.70. These results are comparable to Nemec et al. [37], who stated that quantitative CEUS parameters could provide useful additional information compared with subjective human visual qualitative diagnostic criteria.
Jung et al. [11] described that CEUS perfusion for the evaluation of PE could better differentiate between benign and malignant lesions when comparing the nodules with the surrounding parenchyma. The benign lesions such as adenomas have a prolongated enhancement, which is shown as no visible or only a partial wash out [8]. While the malignancies had lower TTP, revealing a faster and greater microbubbles uptake [38]. According to the quantitative analysis of TICs in this study, the PE, WiR, and WoR were significantly related to malignant nodules, indicating that the enhancement intensity of microbubbles in malignant nodules during the whole stage of enhancement was lower than that in benign nodules. However, we did not find a statistical difference between benign and malignant nodules in TTP. The potential factor may be attributed to the small size of the nodules. In addition, DCE-US and CEUS showed substantial agreement in the diagnosis of malignant and benign thyroid nodules. These results are comparable to a previous study, which achieved a significant difference in enhancement using quantitative analysis of CEUS between benign and malignant nodules (P < 0.001) [37].
Although it was prospective, there were several limitations of this study. First, the number of cases was relatively small. However, the data were collected from two hospitals in Asia and Europe, which reduces the risk of potential bias in data collection. Second, all of the malignant nodules were PTCs. The diagnostic value of DCE-US for other pathological types of malignancies requires further investigation. Third, benign nodules were proven by cytology in this study, and some false negative results may have occurred, affecting the final outcome of assessment. However, the benign results were obtained by repeated FNA, and the risk of false negatives was close to zero, as proven by a previous study [17]. Fourth, DCE-US is not standardized across different manufacturers. Thus, the generalizability of our results is unclear. Fifth, the difficulty in performing the perfusion analysis is that the nodules need to be kept within the field of the ROIs. Therefore, experienced operators are required to hold the probe and the ultrasound image stable for at least one minute. This study showed almost perfect interobserver agreement in assessing CEUS images, which maintained image quality for analysis. Moreover, the sizes of thyroid nodules included in the present study were≤1.0 cm. Additional studies with different sizes of nodules are required to validate the present results.
In conclusion, the results of the present study suggest that VueBox® is a helpful tool for the evaluation of dynamic microvascularization of thyroid nodules, and the DCE-US using VueBox® perfusion analysis could provide added values for differential diagnosis of small solid thyroid nodules (≤1.0 cm).